







A Decongestant Debate That Won’t Clear Up
Randy Hatton ran the hotline. His students fielded dozens of drug-related questions from pharmacists, physicians, and even the occasional vet. When the phones rang, Hatton and his team never knew what to expect. One time, surgeons dropped part of a patient’s skull on the floor and wanted to know what solution would sterilize the bone chunk before they put it back in. Another time, veterinarians called to ask how big of a dose of human antibiotics to inject into an African elephant. But then, Hatton, himself a pharmacist, got a question that sparked a 20-year quest over a seemingly benign drug: a popular over-the-counter decongestant.
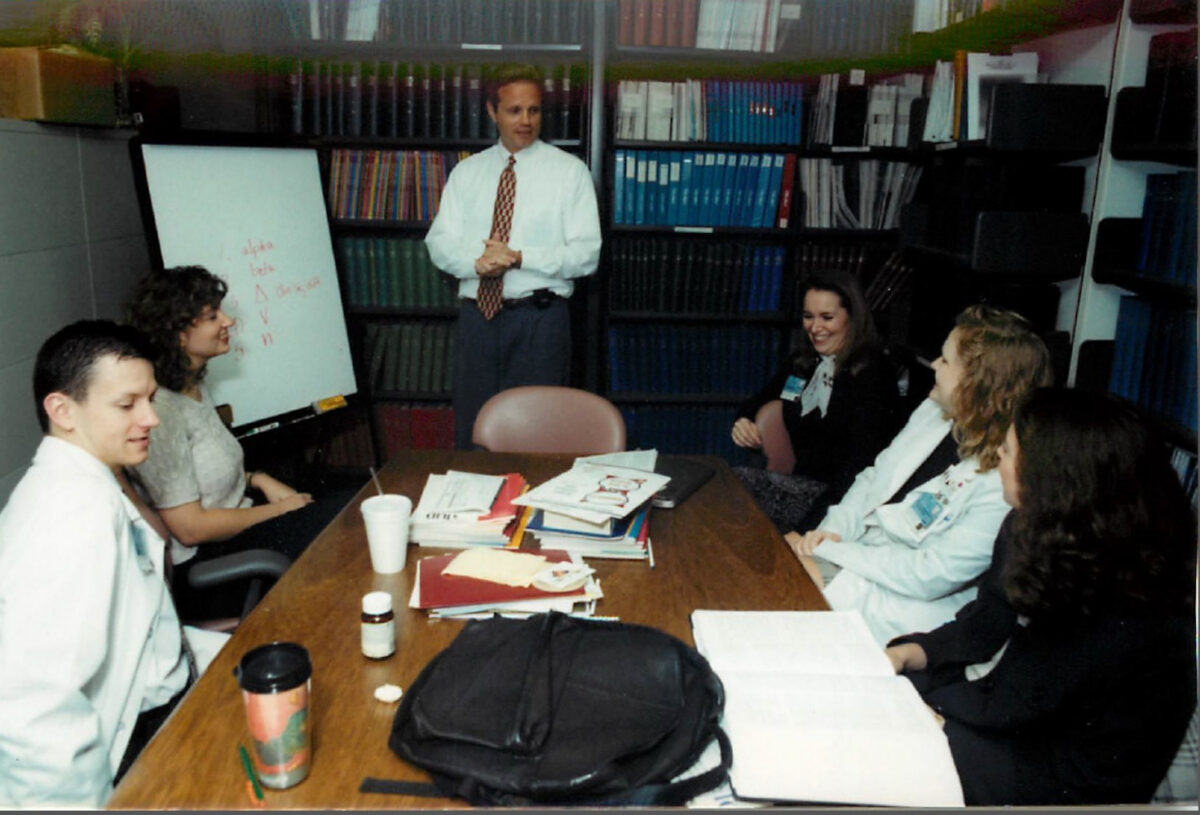
Randy Hatton and post-doctoral pharmacy residents at the Drug Information and Pharmacy Resource Center in the 1990s. The hotline fielded dozens of questions from pharmacists, physicians, and even the occasional vet. Calls about Sudafed PE piqued Hatton’s interest.
Visual: Courtesy of Randy Hatton
Known as the Drug Information and Pharmacy Resource Center, the hotline had been founded in 1972 at the University of Florida in Gainesville. By the mid-2000s, the center had cubicles and functioned as a 9-to-5 training lab for students. (In an era of dial-up and limited internet access, Paul Doering, the center’s former co-director, said, “We were king of the world because we could find stuff.”) Although practitioners could query online databases like PubMed for answers, when they came up short, they put in a call to the hotline. As such, the center tended to get hard questions.
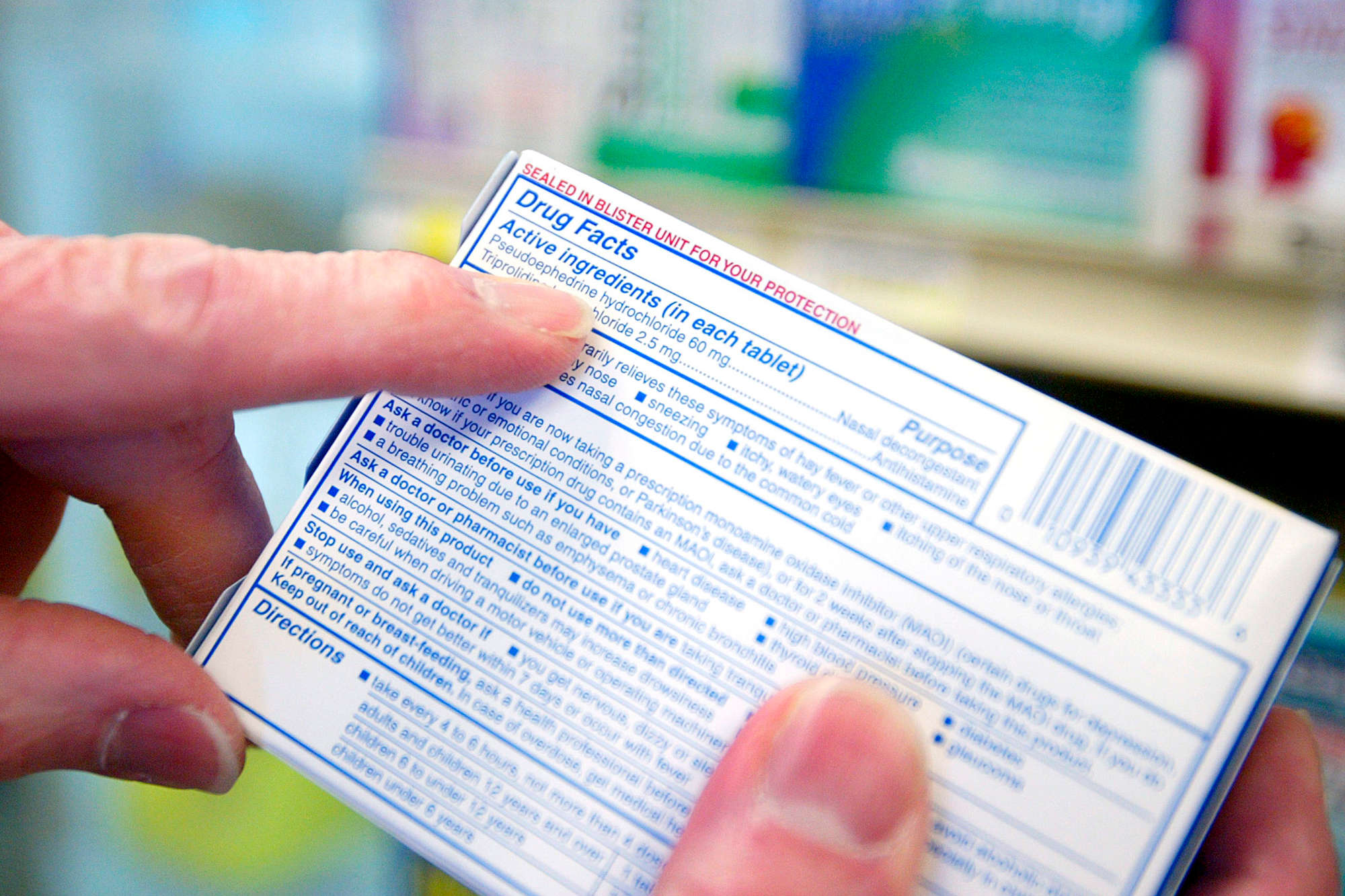
And that’s how the question that really stuck came in. In 2005, callers began sharing a similar anecdote with students working the hotline: People stopped taking Sudafed, the over-the-counter nasal decongestant that regulators had made more difficult to obtain, and started taking its replacement, Sudafed PE. “They would buy it, and they would take it home,” Hatton said in a phone interview. “And then they’d go back to their pharmacist and say, ‘That stuff doesn’t work. What’s wrong? It doesn’t work.’”
On its face, the reformulation seemed subtle. The packaging looked nearly identical, but the newer version had replaced the key ingredient, pseudoephedrine, with another compound called phenylephrine. Soon, though, it wasn’t just his students trawling databases. Hatton himself wondered why the stuff did not seem to do much in the way of clearing sinuses.
It took far longer than he anticipated to figure it out. What ultimately happened — notably, a series of momentous actions by federal regulators followed by apparent inaction — reveals the onerous path to reverse, or undo, a drug approval.
According to the Consumer Healthcare Products Association, a trade association whose members included nine companies involved in the manufacturing and repackaging of oral phenylephrine, half of all U.S. households rely on oral phenylephrine. The makers of Sudafed publicly maintain that the drug is safe. And the CHPA maintains that the scientific evidence supports the drug as an effective nasal decongestant. In an email, Logan Tucker, vice president of public affairs at CHPA, referred Undark to the association’s formal written comments, which state, “Not every drug is effective for every patient or consumer who uses it.”.
What ultimately happened — notably, a series of momentous actions by federal regulators followed by apparent inaction — reveals the onerous path to reverse, or undo, a drug approval.
But lingering questions around the drug’s efficacy might hint at what holds true for a wider range of products, including prescription drugs used to treat cancer, products to treat nausea during pregnancy, as well as other cold-and-cough products, some of which were approved a long time ago. Unlike homeopathic remedies, supplements, or other unproven health care products found at drugstores, prescription drugs and over-the-counter medications bear the imprimatur of U.S. Food and Drug Administration. And medications formally approved for use by the FDA are supposed to be both safe and effective. But it remains unclear how many FDA-approved drugs do not work, and experts say there’s little precedent for how the agency would systematically go about reviewing — and removing — an ineffective drug from the market.
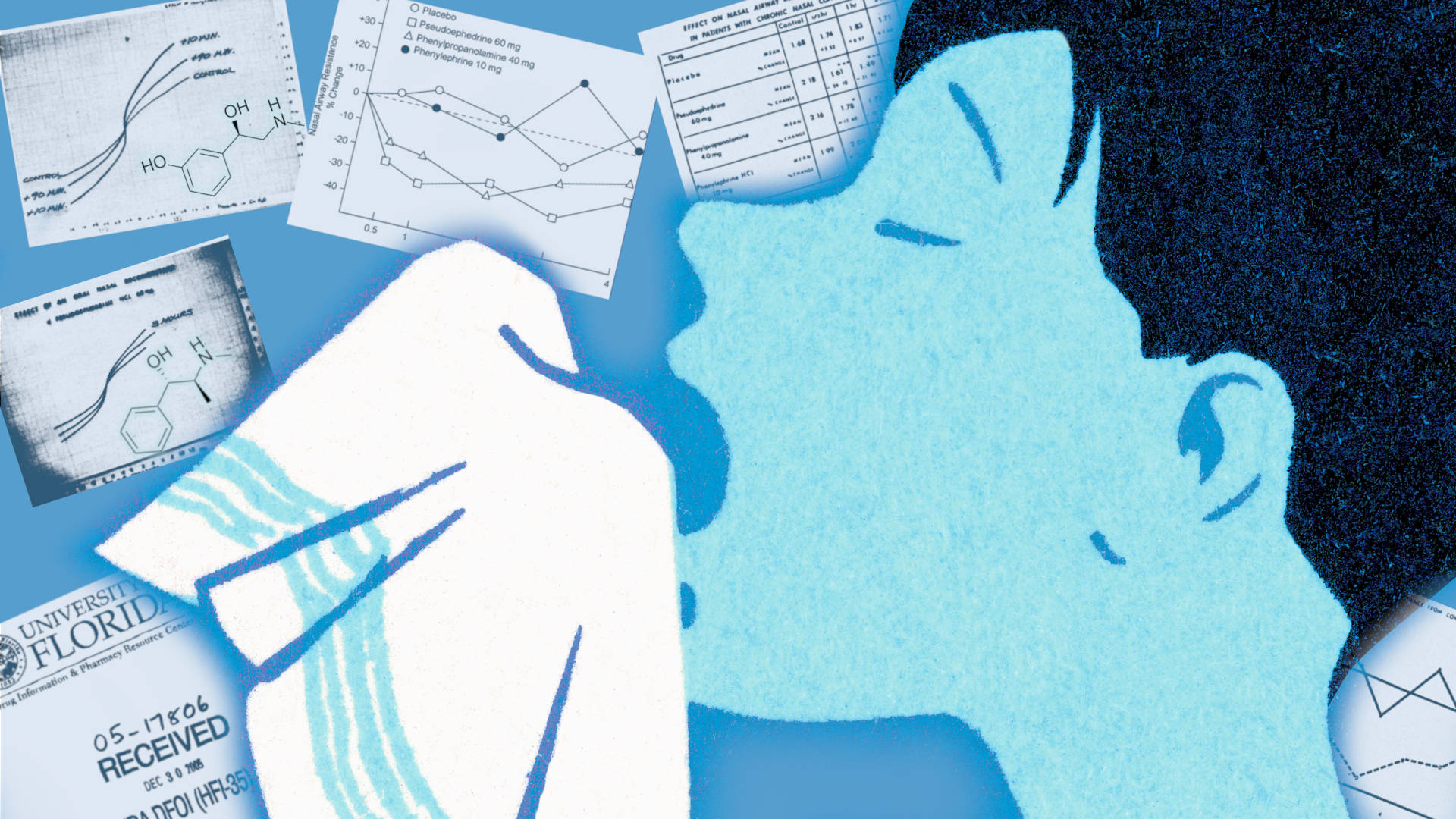
Back in 2005, though, when the phenylephrine questions first surfaced, Hatton wasn’t all that familiar with the ingredient. But he learned that a colleague, Leslie Hendeles, had published a paper on decongestants in 1993. Hendeles also had an office on campus, so Hatton walked over to meet with him. Perhaps even more improbably, Hendeles’ paper had cited a conference proceeding from 1971 — results that the FDA itself initially had not been able to locate.
The two pharmacists did not think the decades-old data looked good. It suggested oral phenylephrine, in 10 milligram doses, was no more effective than a placebo. But the 1971 paper was essentially the only info out there, and it had limitations: It hadn’t been designed to test for efficacy, and it wasn’t even published in a scientific journal. “I can’t tell you the exact conversation that we had,” Hatton said, “but we both had this interest in this issue — because, to me, it’s like, how can this be that this drug is on the market now and it appears that it doesn’t work?”
This had not been a problem up until the mid-2000s. Prior to that, phenylephrine wasn’t in widespread use — at least not in oral form. But lawmakers cracked down on pseudoephedrine, the active ingredient in Sudafed’s original formulation, since it could be made into methamphetamine, particularly the “shake-and-bake” synthesis in soda bottles. The laws obliged pharmacies to keep pseudoephedrine products behind the counter and added other barriers to purchase, which prompted Sudafed’s maker at the time, Pfizer, to find a new ingredient. Other companies quickly followed suit. Manufacturers found alternatives to pseudoephedrine using phenylephrine — the latter of which had already been FDA-approved, could not easily be made into meth and was available over the counter. (A spokesperson for Pfizer did not respond to questions about its effectiveness and said another company now owns the brand. Kenvue, the current owner of the Sudafed brand, did not respond to questions.)
But based on the calls coming into Hatton’s hotline, the new drug didn’t work. “Well, we need to get to the bottom of this,” he recalled telling Hendeles. “And so that led us down the road of a couple of decades’ worth of work.”
Lingering questions around oral phenylephrine’s efficacy might hint at what holds true for a wider range of products, some of which were approved a long time ago.
In the ensuing years, Hatton sat in his office adjacent to the call center. He hadn’t wanted to base his conclusions on a single paper, so, in 2005, he faxed records requests to the FDA. The agency then mailed him typewritten studies, raw data on each of the human subjects from unpublished studies, most of which manufacturers paid to be done in contract labs. Hatton manually entered these data into spreadsheets. (A pharmacy student replicated the data entry process, allowing them to double-check each cell. “That stuff was mechanical,” Doering said.)
The longer Hatton looked, the more his confidence increased: The drug didn’t work. The FDA greenlit the drug in 1976 using data from 14 studies. Hatton initially obtained 11 of them. Of these, four showed efficacy at the 10 mg dose, and these four came from authors affiliated with contract labs. To Hatton, the results seemed a little too pat. (It wasn’t exactly a row of identical digits, but statistically, the number 5 appeared too often in the first decimal place, according to a later analysis.) “They were too consistently what they were supposed to look like,” Hatton said. Except that the placebo flatlined, showing basically no effect, which seemed odd given that placebos can exert an effect so well-known it has a name: the placebo effect.
Hatton’s hunch: The only studies showing phenylephrine worked were, he said, “most likely fraudulent.”
In 1938, disaster prompted Congress to give the newly founded FDA more power. Before then, drug sellers only had to show their products were not contaminated or adulterated. But, after a toxic solvent, elixir sulfanilamide, caused a series of agonizing deaths, regulators required another measure: safety. Almost three decades later, thalidomide, a sedative and treatment for morning sickness, caused severe birth defects which stimulated hearings and another round of reform. It was then that officials homed in on efficacy. In terms of a drug’s pharmacology — that is, its effects on the body — efficacy means its capacity to produce a result.
According to historians Jeremy Greene and Scott Podolsky, efficacy was one of the “least controversial components” of the 1962 Kefauver-Harris Amendments, which required drugmakers to prove that drugs were both safe and effective. The resulting provisions demanded adequate and well-controlled trials. “It’s a landmark event in the history of drug regulation in the world,” said Peter Lurie, former associate commissioner at FDA and now president of the Center for Science in the Public Interest (CSPI), a nonprofit advocacy group in Washington. “No other country had that efficacy requirement until then. It was a big deal, and it remains so.”

Because some ingredients had squeaked by prior to 1962, the agency went back and reassessed efficacy for drugs approved prior to the amendments. The so-called Drug Efficacy Study Implementation process took years, and hundreds of drugs came off the market as a result. But not everything that remained was necessarily tested with appropriately designed clinical trials. As Doering put it, “phenylephrine came along at a period of time where those, I guess you could say, were just clouds in the sky.”
Members of the public can and do submit case reports directly to FDA. In recent decades, the most common report to the FDA’s Adverse Event Reporting System is “DI”: drug ineffective. These events are also most commonly reported by patients, rather than healthcare providers or other drug manufacturers. (The system was recently consolidated.) But U.S. regulators rarely hit undo unless there is some indication that the drug is unsafe. According to a 2005 paper, more than 75 drugs — 1 percent of all those marketed since 1969 — were removed in the previous 33 years, almost all due to safety concerns. The reasons efficacy rarely forces a product off the market is that once it’s been proven, Lurie said, there’s little incentive to redo studies. “All they’re going to get is bad news, right? It’s not very likely that the next trial is going to show their product to be even more efficacious than thought.”
“How can this be that this drug is on the market now and it appears that it doesn’t work?”
The risks may seem low in terms of causing harm, but researchers raise concerns around efficacy for several reasons. It adds unnecessary costs for consumers; as many as one in five drugs newly approved in the U.S. between 2017 and 2020 failed to demonstrate benefits in other countries, for instance, and were not approved by foreign regulators. With regards to phenylephrine, specifically, a group of researchers led by Timothy Anderson, a physician at the University of Pittsburgh who co-directs the Prescribing Wisely Lab, suggested in a 2024 study that FDA needed to hold over-the-counter drugs — those available without a prescription — to a higher standard. In a press release about the study, he acknowledged such a proposal would be a tall ask: “This will require a substantial investment in infrastructure to expand capacity.”
The case of oral phenylephrine has its peculiarities, Stanford University’s John Ioannidis and Sarah Tanveer, two experts in how research is conducted, wrote in a 2025 commentary, but the data on phenylephrine prompted broader issues around the removal of ineffective drugs. Indeed, their commentary asked: “How should regulators prioritize removal of ineffective products?” The steps forward remain unclear. “They have to go through a lot of, I would say, regulatory bureaucracy to remove a product from the market,” said Tanveer in a phone interview. “And now things have changed so much with the current administration. They’re not exactly following all of the prior rulemaking processes.”

At the same time, Tanveer and others argue, evidence standards have diminished, requiring fewer trials and making it easier to get a drug approved. Indeed, Lurie suggested that current administration officials seemed determined to unwind the regulatory clock to 1938. “What you would end up with is a Wild West of people making claims again, and no real way to police them because there’d be no requirement to show effectiveness,” he said. “You just have no way of knowing if it worked.”
In some ways, there had never been exactly a playbook for removing drugs with questionable or nonexistent efficacy, despite lack of effectiveness being the most common adverse event consumers send to the FDA. The process was not exactly well-defined, and, as the story of phenylephrine goes to show, marked by uncertainty.
In 2006, Hatton and Hendeles published the first letter about their findings. Then, they published a meta-analysis, combining all the data Hatton obtained from the unpublished studies. But they did not stop there. They contacted the FDA (“naively,” the two later wrote.) The agency took no action, but told them to submit their concerns via a citizen’s petition. And so, in 2007, along with another University of Florida colleague, Almut Winterstein, the group filed a petition — the process by which individuals and organizations formally ask the agency to take, change, or stop a specific regulation. These petitions are usually rejected. (In a 2018 paper, three scholars from the University of California Hastings College of the Law wrote that pharmaceutical companies have “hijacked” the process, using petitions to maintain market exclusivity; even if a petition fails, it can nonetheless delay a rival product, generating “hundreds of millions of dollars in revenue for a blockbuster drug,” the authors wrote.)
Hatton maintains he had no financial stake in the outcome: “The incentives have been just the opposite,” he said. “We spent a lot of our own personal time doing this. None of this, none of this activity was funded in any way.” And so it was against the odds, and with a little help by one member of Congress writing letters to the FDA encouraging an evaluation of phenylephrine, when the agency scheduled a hearing in February of 2007 to discuss phenylephrine’s lack of efficacy. It was a real milestone, Hatton said, but he had no money to get to Washington, D.C.

Instead, Hendeles presented in person at an FDA advisory committee meeting later that year. Hatton presented remotely via video. As the meeting plodded on, Hendeles boiled down their petition: Phenylephrine was no more effective than a placebo. “If you have a stuffy nose and you take Sudafed PE,” he said according to a meeting transcript, “you’re going to still have a stuffy nose.” When Hatton presented, one of his slides hinted at the alleged fraud. “Only one laboratory,” he said, “Elizabeth Biochemical, provided consistent evidence of positive results for oral phenylephrine.” When Winterstein brought it up a second time, it got a rise out of the committee’s industry representative.
“That’s an accusation that comes out of the sky as far as I’m aware,” an executive at Martek Biosciences told attendees, according to the meeting transcript. “I mean, is there ever — is the FDA, is there any issue that’s ever been raised about these studies that would even suggest that this should be brought up publicly?” Hatton couldn’t see the guy, but he could hear it in his voice: “I mean, he flipped out.” (Martek no longer exists; the executive could not be reached for comment.) The meeting ended without resolving that issue, or the bigger underlying question as to whether phenylephrine was effective. The committee concluded that more data were needed.
Years passed. Looking back, Hatton isn’t sure why he persevered, but it was as if he kept catching faint glimmers of daylight through the cracks of an otherwise impenetrable wall. One drug company, Schering-Plough (since acquired by Merck), funded additional studies co-authored by company scientists, got negative results, and published them. Six years later, another study, also with contributions by Merck, added to the evidence against efficacy. (In response to requests for comment from Undark, the corresponding authors listed on these papers either declined to comment, did not respond, or could not be reached.) Phenylephrine is metabolized in the gut, meaning, in terms of bioavailability — the extent to which a drug reaches its destination — almost none of the active ingredient likely reached the nose at the 10 mg dose.
As the meeting plodded on, Hendeles boiled down their petition: Phenylephrine was no more effective than a placebo.
In 2015, Hatton and Hendeles withdrew their original petition and filed a new one. Only this time they not only got a hearing date, but they also apparently found a more sympathetic ear: Theresa Michele, who was then head of Office of Nonprescription Drugs. (Michele did not respond to a request for comment.) According to Hendeles, “she let the data guide her rather than politics.” In advance of the 2023 meeting, Hendeles downloaded the briefing document. The medical officer the FDA brought in, and the interdisciplinary team of scientists he worked with, had sided with the crusading pharmacists. Peter Lurie, the former FDA official now at the nonprofit CSPI, said, “You barely have to read between the lines in that document.” (Lurie has since filed a formal comment with Hendeles and Hatton on the FDA’s proposed order.) In Lurie’s view, the document spelled it out clearly: “This product doesn’t work. It can’t work. It never worked.”
The briefing document flagged a set of studies the FDA had originally relied upon to approve phenylephrine, which came from Elizabeth Biochemical, as “too good to be real” and “highly problematic.” The reviewers added that their red flags went up independently — that is, they noted methodological and statistical issues prior to knowing about Hatton and his colleagues’ published allegations. In a comment that was later redacted, the reviewers said such results would prompt an investigation, but added, “Fifty-plus years later, that is impossible, so at this point all we can do is report our suspicions.” The author named on the Elizabeth reports could not be located, and neither the trade group CHPA nor Kenvue, the drug company that currently markets Sudafed, responded to emailed questions about the allegations at the Elizabeth study site. But, in its 2023 comments to FDA, CHPA disputed these claims: “it is not appropriate to speculate that data integrity issues are the underlying reason for failure to replicate efficacy results without any substantiating evidence backing up the assertion.” The allegations of fraud remain unproven.
Nevertheless, when the advisory committee met again in 2023, Hendeles said: “I knew that the people that had done the investigation internally had come up with the right answer. So I was not surprised.” He watched the proceedings remotely, and when the committee voted, he said, “I was ecstatic.” Hatton, watching alone at his home office, said the committee’s unanimous vote in favor of removing phenylephrine confirmed a hunch. “It vindicated our position all along.” The vote made a splash. The advisory committee recommended taking the next step, which meant preparing a docket for public comments followed by a final ruling. Both Hatton and Hendeles spoke with a reporter at NPR. Hatton appeared on PBS. The American Society of Health-System Pharmacists, the publishers of AHFS Drug Information, the desktop reference book, illustrated its news story with a figure rolling a Sisyphean boulder up a hill. The New York Times ran an op-ed by the two pharmacists. One national chain drugstore, CVS, pulled phenylephrine off their shelves (but not products that include phenylephrine in combination with other active ingredients). A law firm retained Hatton as a witness, but the suit was dismissed — in large part, he said, because phenylephrine was still FDA-approved. The lawsuit has since been appealed.
In the end, Sudafed PE and other decongestants containing phenylephrine remain on the market. Phenylephrine makes up the single largest share of over-the-counter nasal decongestants, and sales generate more than a billion dollars annually. In its formal 2025 comment to FDA, the CHPA refers to an unpublished 1975 study as “the largest cold study,” and took issue with claims made by the FDA’s scientific reviewers that the study’s methodology was biased; the comment said the reviewers’ description of the subjective scoring used in the 1975 study was “misleading.” The comment reiterated the industry’s position: “The assertion that there is no clinical data demonstrating the effectiveness of oral phenylephrine is not accurate.”
In some ways, there had never been exactly a playbook for removing drugs with questionable or nonexistent efficacy, despite lack of effectiveness being the most common adverse event consumers send to the FDA.
In recent months, President Donald Trump has launched efforts intending to bring down drug costs. Officials have signaled that they want to accelerate approvals, making more drugs over the counter, while also adding additional safety reviews for other therapeutic interventions, such as childhood vaccines. (“But then the secretary, on the other hand,” Lurie said, “seems to want to open the floodgates to stuff that nobody has ever convinced FDA worked: dietary supplements, peptides — God knows what else — bleach?”) Federal authorities have made no apparent statement on the long-awaited final order. The former head of the division overseeing the decision, Michele, who spoke publicly in favor of removing oral phenylephrine, was reassigned at the end of 2025, according to Reuters and STAT. There is no statutory time limit for final orders, but the pending removal seemed to be in limbo. “We don’t know what’s going on right now,” Hatton told Undark.
Tracy Beth Høeg, the acting director of the FDA’s Center for Drug Evaluation and Research, did not respond to an emailed request for comment, and an unnamed Health and Human Services spokesperson said the agency could not comment on forthcoming regulatory decisions. The proposed order received nearly 3,000 comments. In Hatton’s view, none of the comments said: “Here’s new evidence that shows that it works.” Nonetheless, some patients swore by phenylephrine. In its statement, the spokesperson confirmed the agency’s process involved a review of comments, which meant FDA could issue a final order to remove oral phenylephrine any day. If the agency does not order its removal, Hatton and Hendeles still have another shot at proving their case in court.

In its survey showing that 50 percent of U.S. households rely on phenylephrine, the CHPA’s formal comments to FDA note that more than two-thirds of these were repeat customers, which “suggests the purchaser found its effect sufficient to warrant another purchase.” The CHPA warned of major disruptions should the products get pulled from shelves.
Hatton’s quest raised questions about drug efficacy, and about the regulatory process to assess it, especially once a drug had passed the FDA’s efficacy and safety requirements. In their 2024 paper — titled, “What We Have Learned From Trying To Remove Oral Phenylephrine From The Market” — Hatton and Hendeles wrote that the process was slow. It got political. The two took issue with those who implied that keeping drugs on the market offered consumers a choice. An ineffective drug wasn’t a choice, Hatton said. “It’s crazy how long it can stay on the market,” he added. “But if you’re making billions of dollars a year, every month is a lot of money to the manufacturers who have those drugs. So I’m sure they have used whatever clout they have to try to slow this process down.”
When asked about the predicted shortages, Hendeles was more to the point: “It’s bullshit.” In the mid-2000s, the whole question around its efficacy started when drugmakers replaced pseudoephedrine with phenylephrine, demonstrating that manufacturers could quickly reformulate, Hatton said, “Because it was in their economic interest to do it.”
As a retired organic chemist with loads of allergies and a father who was a patent lawyer with connections to the early work on modifying amphetamines to make better decongestants with Smith Kline pharma, I have some important thoughts on the decongestant and other maladies involved with these drug structures and treatments
I have found that phenylephrine IS an effective medication at 10 mg every several hours. I get bad colds and allergy attacks, and its use is good for me in pills and also nasal mist. I think it’s being attacked because it’s cheap and the Big Pharma firms want to sell the public stuff that’s more expensive with higher markup, instead of the old lower-profit phenylephrine products.