






Shortly after assuming office, President Donald Trump announced broad cuts in foreign medical, food, and other aid. This included gutting the United States Agency for International Development (USAID) and significantly disrupting the President’s Emergency Plan for AIDS Relief (PEPFAR) — a 22-year-old program active in dozens of countries. The cuts are already impacting lives across the globe, with one Boston University analysis anticipating hundreds of thousands of excess fatalities caused by HIV/AIDS, tuberculosis, malaria, and other diseases.
In March, reports began to emerge that the Trump administration was also exploring cuts domestically. This has included slashing the number of HIV branch offices overseen by the Centers for Disease Control and Prevention, and cuts to hundreds of federal grants — representing hundreds of millions of dollars — to health departments, universities, and nonprofit organizations doing work in the HIV/AIDS space. At least 230 HIV-specific National Institutes of Health grants have been canceled.
Broadly, the Trump administration’s reasons for grant terminations include that they’re misaligned with agency priorities, which could mean research areas considered problematic or work conducted overseas. Speaking with Undark, Jeffrey Klausner, a professor of medicine and global health at the University of Southern California, described two HIV-related grants of his that have been canceled: One on the grounds that a transgender population was involved and the other because subjects included in the research were based in Peru and not the U.S.
At least 230 HIV-specific National Institutes of Health grants have been canceled.
Meanwhile, the White House’s proposed budget for 2026 would further reduce discretionary spending within the U.S. Department of Health and Human Services by 26 percent, including cuts to nearly $18 billion in funds for the National Institutes of Health. In addition, Trump’s plan almost halves the CDC budget. The administration says it wants to cut waste and inefficiency in federal spending and what it perceives as programs focused on diversity, equity, and inclusion. While Congress must still approve the final budget, Colleen Kelley, chair of the HIV Medicine Association and Associate Professor of Medicine, Division of Infectious Diseases at Emory University, warned in a statement that “drastic cuts to HIV public health and research programs proposed in the president’s budget would leave America’s HIV response in peril if enacted.”
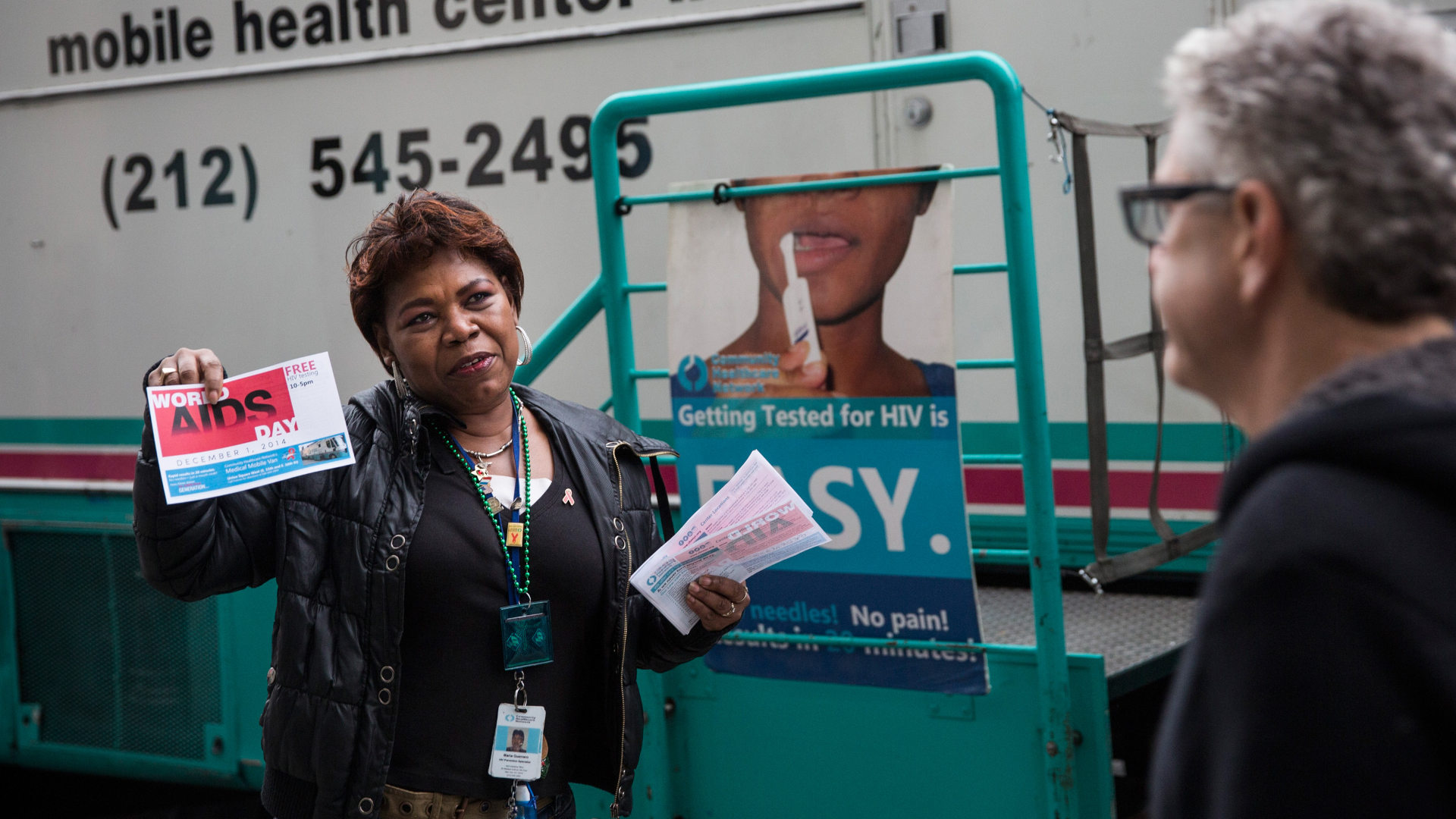
At a minimum, the myriad cuts seem likely to jeopardize recent successes in addressing the nation’s HIV epidemic, including those related to the Ending the HIV Epidemic Initiative, which was established, ironically, under the first Trump administration. This initiative coincided with a 12 percent decline in new HIV infections nationally from 2018 to 2022. The CDC stated that preventive measures such as “increases in preexposure prophylaxis prescriptions, viral suppression, and HIV testing likely contributed to the decline.”
While KFF says that despite the cutbacks, “most but not all of the nation’s HIV care and treatment safety net” would be maintained, federal HIV prevention efforts will nevertheless be forced to scale back substantially, suggesting that declining infection rates might well reverse direction. According to estimates from the Foundation for AIDS Research, for example, slashing federal funds for HIV prevention could result in approximately 143,000 additional people in the U.S. becoming infected with HIV within five years, and about 14,700 more individuals who die of AIDS-related causes.

Klausner suggested that cuts to HIV prevention would hamper community outreach efforts, which, for example, may lead to vulnerable populations not accessing preventive PrEP medications. This could then result in more spread of the disease.
For its part, Trump’s HHS defends the cuts on the basis of increased efficiency and shifting priorities. In a roundtable interview last month, NIH director Jay Bhattacharya described grant cuts and other cutbacks at the agency as part of HHS secretary Robert F. Kennedy Jr.’s desire for increased focus on chronic diseases in addition to infectious ones. Secretary Kennedy in turn has spoken of the need to reduce waste and duplication. He said in a Congressional hearing on May 14 that the department intends to focus on chronic disease and “to do more, a lot more with less.”
And that’s where the logic of the administration’s approach to HIV research and prevention funding seems to fall apart. HIV, after all, is a chronic disease for the approximately 1.2 million people in the U.S. living with it. The disease is manageable for patients with the right antiretroviral medications, and these pharmaceuticals have evolved over time. Advances in treatments include new classes of drugs, new formulations of existing treatments, preventive medicines such as PrEP, and long-acting antiretroviral drugs. Additionally, there are mRNA vaccines for HIV in development. Two years ago, researchers published encouraging first-in-human results demonstrated in early-stage clinical trials.
Continued progress in HIV/AIDS medicine, whether related to prevention, treatment, or research, is contingent to a considerable degree on public funding, and in particular, federal government resources. State and local health departments depend on the CDC for their funding. In fiscal year 2023 alone, the agency committed nearly $15 billion to state and local health departments.
Theoretically, states and municipalities could replace a portion of the federal cuts in HIV prevention. But a limiting factor is the fact that some, particularly in the south, spend little or nothing of their own money on things like HIV prevention. In addition, states could soon be confronted with cuts in federal funding of the joint state-federal insurance program, Medicaid, which covers 40 percent of the HIV population.
Slashing federal funds for HIV prevention could result in approximately 143,000 additional people in the U.S. becoming infected with HIV within five years.
According to Scientific American, drug companies such as Gilead Sciences and GSK “that produce HIV drugs are among the largest contributors of non-governmental funds for HIV testing, prevention, and care.” But such funding is considerably less than the roughly $43 billion that the federal government allocates to HIV annually. And while private foundations can fill in some of the gaps, they have limited resources compared to the federal government.
In a statement to the Infectious Diseases Society of America, Kelley described HIV research as “one of the most powerful examples of the return on investments made by NIH. It is because of NIH funding that there are incredibly effective options for treating and preventing HIV.” Meanwhile, the scientific and medical personnel and infrastructure needed to sustain these gains will collapse, Kelley warned, without sufficient funding.
It remains to be seen, of course, whether HIV prevention, treatment, and research will indeed crumble due to already implemented and planned cuts by the administration. What’s clear is that public health related to HIV faces unprecedented financial challenges at home and abroad, and these will be exceedingly difficult to overcome.