







Six years ago, in the summer of 2020, I began my emergency medicine residency in Atlanta and started one of the most traumatic first years of training I could have imagined. As Covid-19 patients overwhelmed the hospital where I worked, I watched colleagues burn out. I watched patients die alone. I watched a healthcare system that I had spent my entire life preparing to work in buckle under the weight of something none of us were prepared for.
So when the headlines about a hantavirus outbreak on a cruise ship started flooding my phone a few weeks ago — with friends panicking and family members asking if this was another Covid — I understood the fear immediately. That fear is not irrational. It is the residue of collective trauma we have never properly processed.

Based on what we know about hantavirus, this outbreak is extraordinarily unlikely to become a pandemic. The real story of the virus, however, has nothing to do with a cruise ship.
I now work as an emergency room physician on Martha’s Vineyard. But several times a year I also work on the Navajo Nation, a reservation in the Four Corners region of the American Southwest, where I have personally cared for a patient with hantavirus. It is a devastating illness. You watch someone who initially presents with what they thought was the flu deteriorate into acute respiratory failure faster than almost anything else in emergency medicine. There is no cure. There is no specific treatment. You support their body, and you hope.
In the U.S., hantavirus disproportionately kills Indigenous people. According to a Centers for Disease Control and Prevention report based on data from 2007 to 2011, Native Americans experience hantavirus pulmonary syndrome at least 10 times the rate of White Americans, one of the largest racial disparities among notifiable diseases in CDC surveillance. When they get it, they die from it more often, and they are younger when they do.
The reasons are structural: rural geography, housing conditions shaped by decades of federal disinvestment, and higher burdens of diabetes and cardiovascular disease that make any severe infection deadlier.
Based on what we know about hantavirus, this outbreak is extraordinarily unlikely to become a pandemic. The real story of the virus, however, has nothing to do with a cruise ship.
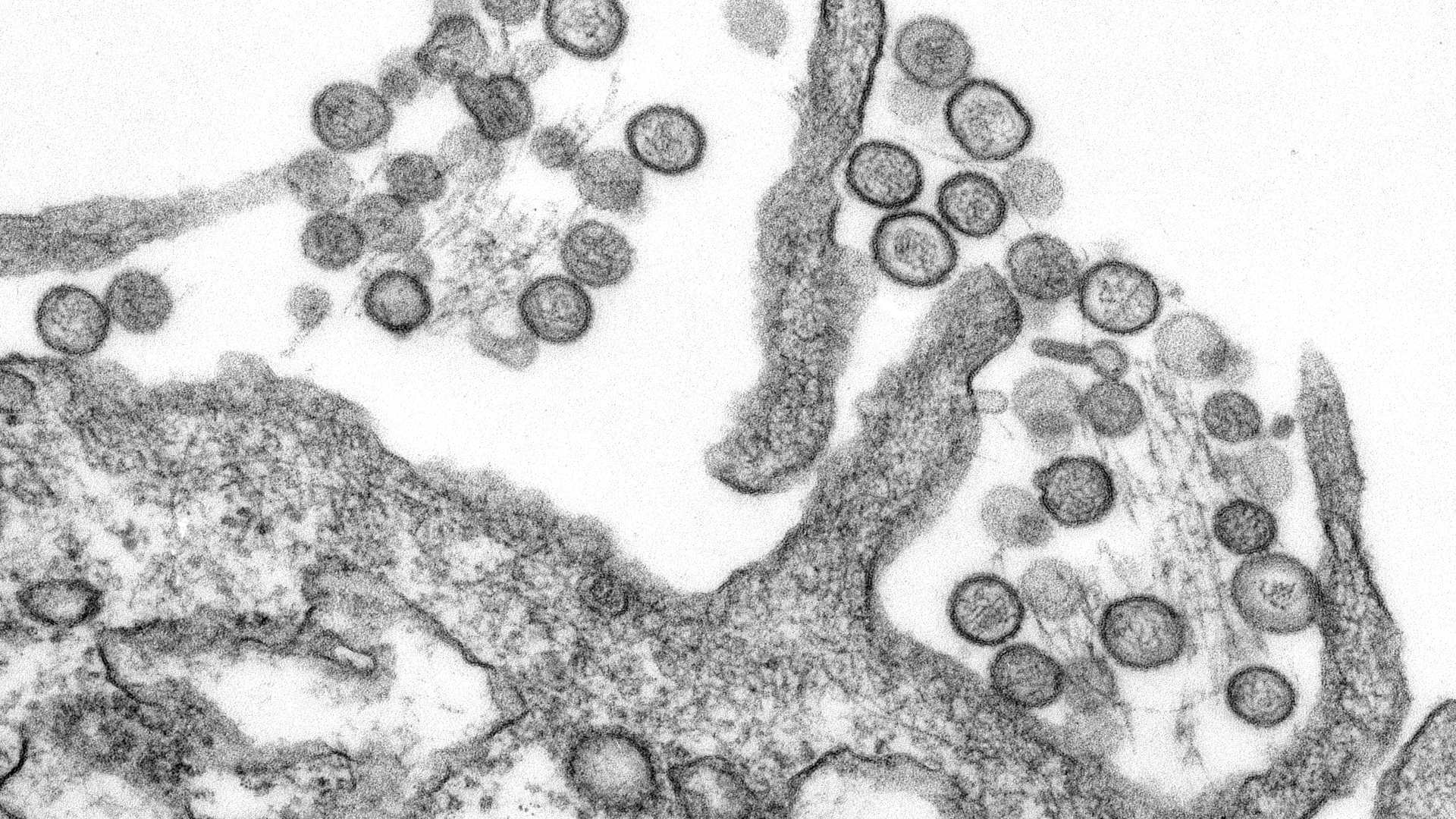
Hantavirus does not spread through the air between people the way influenza or SARS-CoV-2 (the virus that causes Covid-19) does. People usually get it from rodents — their urine, their droppings, and their saliva, which can be stirred up into the air and inhaled. The Andes strain found aboard the cruise ship MV Hondius is the one exception: It is the only hantavirus known to transmit person-to-person (via droplet and airborne routes), and even then, that transmission typically requires prolonged close contact.
Epidemiologists measure a virus’s spread using the basic reproduction number, R0, which indicates how many people, on average, one infected person passes the virus to. For Andes virus, that number is around 2 — lower than measles and Covid-19. There is no evidence to suggest that the Andes virus is mutating, and it is not a novel virus; it has been studied for decades. The World Health Organization has assessed the global risk to public health to be low.
What concerns me more than the virus is what the panic reveals. We are in a moment of profound medical mistrust, and that mistrust is not baseless. The infamous Tuskegee syphilis study enrolled Black men in Alabama under false pretenses and then withheld effective treatment for 40 years — an experiment conducted not by rogue actors but the official public health apparatus of this country. Black patients are still undertreated for pain compared to White patients; the evidence is unambiguous. Science has historically centered the powerful and experimented on the vulnerable. The grievances are real.
But when we collectively abandon trust in medicine and public health, it is never the powerful who bear the cost. And we are making that abandonment easier than ever: The U.S. has withdrawn from the WHO, and the leaders of this country openly dismiss scientific consensus. The institutions are weakening precisely when we need them most.
In May 1993, when an outbreak of a mysterious respiratory illness struck the Four Corners, the CDC investigators who arrived faced a puzzling challenge. The illness was killing young, healthy people. But the Diné elders had seen this before. (The Navajo people call themselves Diné.)
Navajo oral history had described similar disease outbreaks in 1918 and 1933. According to Navajo surgeon Lori Arviso in her 1999 book “The Scalpel and the Silver Bear,” healers had mapped the entire epidemiological chain: Wet years brought piñon nut abundance, abundance brought deer mouse population booms, booms brought disease. One medicine man, Andy Natonobah, described a treatment ceremony passed through generations involving herbal medicines with inotropic properties (compounds that strengthen the heart’s contractions), adjusted to the patient’s respiratory status over four days. He was describing, functionally, an intensive care unit protocol that had likely been developed before there were ICUs. Arviso, who cared for patients during the outbreak, wrote that Natonobah told one CDC worker to “look to the mouse.”
That knowledge helped crack the mystery, identifying the cause of the outbreak as hantavirus — the first time it was identified in humans in the Western hemisphere and the first time it was found to attack the lungs rather than the kidneys. The CDC’s current web page on reported cases of hantavirus makes no mention of this Indigenous-informed history.
At the time, the media called the disease the “Navajo flu.” Universities began requiring Native American students to undergo medical screening before setting foot on campus. The Washington Post reported that restaurants servers didn’t want to touch Diné customers’ dishes. Tourism collapsed. An already fragile economy took a direct hit.
When we collectively abandon trust in medicine and public health, it is never the powerful who bear the cost.
The virus, of course, did not discriminate: Non-native patients were among the cases, and by year’s end, cases had appeared in 14 states, including Texas, Nevada, Montana, and Kansas. It ended not with a vaccine or cure but with basic rodent control guidance and a natural decline in the deer mouse population. The virus had no way to spread between people. Without that, it ran out of hosts. The same media that briefly credited Diné healers moved on. The community was left with the stigma.
That stigma did not evaporate. It calcified into even more institutional mistrust that made Indigenous communities more vulnerable in every outbreak that followed. During the H1N1 flu pandemic in 2009, Native Americans were among the hardest-hit populations in the country but also hesitant to engage with federal health messaging. During Covid-19, vaccine hesitancy in some tribal communities was not ignorance. It was a historically rational response to institutions that had repeatedly failed them, stigmatized them, and walked away.
We are watching the same cycle begin again. Institutional failure breeds mistrust. Mistrust breeds misinformation. Misinformation breeds panic. And panic, unchecked, always lands hardest on the people already carrying the most.
The hantavirus on that cruise ship is not going to kill us all. But that cycle might.
Prem Menon, M.D., M.P.H., is an emergency physician at Martha’s Vineyard Hospital and Sage Memorial Hospital in Navajo Nation. He is also a researcher at the Harvard Humanitarian Initiative.
It’s very interesting tolearn about rodents and this 1993 break -0ut of Hannnanicus flu , supposedly with native Indians.And we were so overwhelmed – with covid- 19 in January 1, 2020 .