






Experts Raise Questions Over ‘Scary’ Covid Heart Studies
On July 27, the academic journal JAMA Cardiology published a paper showing that 78 out of 100 study participants had abnormalities typically seen in a potentially life-threatening heart condition. Their hearts had been imaged roughly two months after testing positive for SARS-CoV-2, the virus that causes Covid-19. And while two-thirds of the group had suffered mild or no symptoms, medical scans showed fluid and scarring — signs of heart inflammation, or myocarditis.
These findings, among others, “indicate the need for ongoing investigation of the long-term cardiovascular consequences of Covid-19,” wrote the authors, who are based in Germany at University Hospital Frankfurt.
Not everyone was impressed with the paper. The day after it published, scientists identified statistical errors, which the research team went on to correct. Another noted that the study’s controls — people who hadn’t been infected with the virus — also showed inflammation on their heart scans.

But those conversations were unfolding among small groups of scientists on Twitter. Meanwhile, colleges across the country struggled with a vexing question: Was it safe to move forward with fall sports? The study caught their eye because of the rare but devastating possibility of sudden cardiac death in athletes and soon, high-profile media outlets were credulously citing the study as one of the hurdles for a fall season.
An Aug. 8 article in The Washington Post referred to the findings as “bad news for everyone in a general way and scary news for athletes in a specific way.” On Aug. 11, in what would be a highly contentious decision, the Big Ten Conference announced it was postponing its fall season due to ongoing concerns related to the pandemic. The conference later issued a statement on the postponement, which read, in part: “While the data on cardiomyopathy is preliminary and incomplete, the uncertain risk was unacceptable at this time.” Around the same time, Pac-12 announced it would postpone its season as well, in part due to similar concerns.
But over the course of roughly a dozen Undark interviews with physicians and researchers specializing in cardiac radiology, cardiac pathology, and sports cardiology, several expressed concerns over the limitations of the German research, and with a more recent heart imaging study published by a team at The Ohio State University. Some also shared deep misgivings about how the findings of these small studies are being interpreted, reported, and used in the wider world. September’s media coverage has been more circumspect, but these preliminary findings are already being used to guide treatment of virus-positive athletes.
While the experts agreed that Covid-19 can harm the heart, the severity and frequency of the outcomes, as well as how to test for myocarditis, is under fierce debate.
The Big Ten and Pac-12 have since reversed course, with plans to resume their seasons this fall, but the implications of this new research go beyond football. Many experts worry about broader, graver consequences, including the overuse of the pricey heart scans — known as cardiac MRI — and unduly frightening Americans, both of which, they say, could jeopardize public trust in science.
Michael Ackerman, a genetic cardiologist at the Mayo Clinic who has no professional ties to any of the college sports conferences, took issue with the “spookiness” that was being assigned to myocarditis. “If this is the reason why a conference is shutting down a sport,” he said, “I call nonsense on that.”
Even prior to the pandemic, sports medicine physicians were sensitive to the potentially devastating effects of heart problems in athletes. In 1990, Loyola Marymount University basketball player Hank Gathers collapsed on the court during a game and died shortly after. While he had been previously diagnosed with an abnormal heartbeat, an autopsy found he died of cardiomyopathy, a heart muscle disorder, with myocarditis. In 1993, tragedy struck again when Boston Celtic Reggie Lewis died during a team practice under similar circumstances. Though instances of sudden death in athletes are rare, “the outcome is such a drastic one in an otherwise healthy young population,” said Ella Kazerooni, a radiologist at Michigan Medicine who has been coordinating coronavirus testing for University of Michigan student-athletes. For this reason, teams try to stay on top of information about cardiac diseases and screening recommendations.
Myocarditis, in particular, is an important cause of abnormal heartbeats, or arrhythmias, and sudden cardiac death in physically active individuals. The condition is often triggered by a viral infection — it tends to spike seasonally with the flu season. In the early months of the pandemic, case reports and autopsies of hospitalized patients showed that the coronavirus can damage the heart. These findings helped motivate the German and OSU researchers to investigate further.
In May, the American College of Cardiology’s Sports and Exercise Cardiology Council recommended that athletes with positive coronavirus tests should rest for at least two weeks, regardless of whether they have symptoms. Current guidelines from the American College of Cardiology and the American Heart Association also state that anyone with cardiac symptoms, such as chest pain or labored breathing, should undergo preliminary testing to check the heart’s structure and function. Additionally, a common laboratory test measures a heart protein called troponin, which releases into the bloodstream when the heart is damaged.
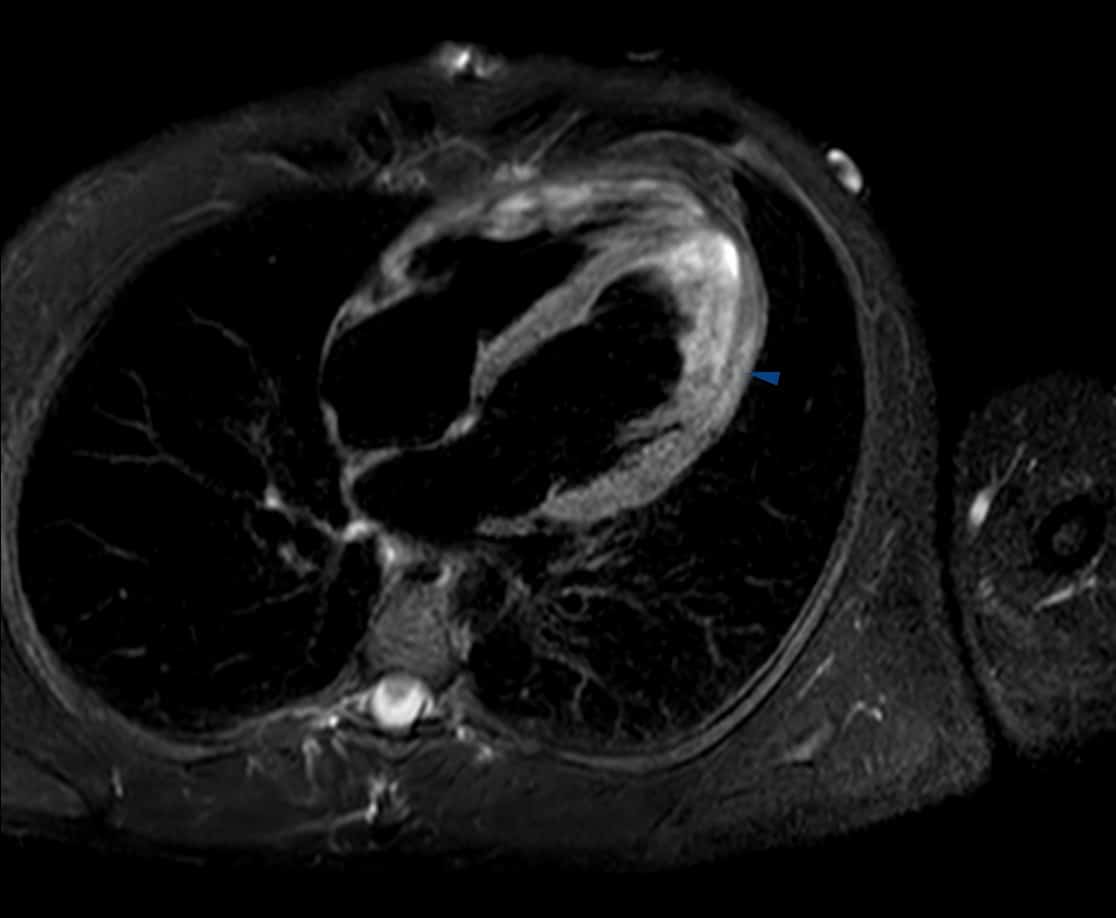
If any of these initial tests turn up abnormalities that suggest myocarditis, a cardiac MRI can help confirm the diagnosis. The MRI produces black and white scans, which can be used to create a 3D view of the heart muscle. It’s among the best tools for identifying inflammation and scar tissue. Cardiac MRIs are rarely used on people who don’t have heart-related symptoms. But the German and OSU studies have prompted some patients and doctors to ask whether the scans should be used more often.
The German study compared three groups of patients: people who tested positive for the coronavirus; people who never contracted the virus and were healthy; and people who never had the virus, but had health issues such as diabetes and hypertension. This third group was included to help disentangle Covid-19 abnormalities from abnormalities that may have been caused by other health conditions — a process called risk matching.
In interviews with Undark, experts offered divergent views of the results, such that the results started to take on the quality of a Rorschach test. “Unfortunately, there is substantial subjectivity in the interpretation of many advanced medical imaging studies, including cardiac MRI,” Venkatesh Murthy, a cardiologist and expert in cardiac imaging at Michigan Medicine, wrote in an email. And when it comes to heart scans of people who are post-Covid and lacking symptoms, he said physicians really don’t know which abnormalities are benign and which are a cause for concern.
Several physicians said they weren’t surprised by the presence of inflammation in study subjects who tested positive for coronavirus. That’s common in people who have just recovered from a viral infection that causes a lot of inflammation, said Chetan Shenoy, a cardiologist and expert in cardiac MRI at the University of Minnesota Medical School.
James Carr, the current president of the Society for Cardiovascular Magnetic Resonance and a radiologist at Northwestern Medicine, said that he finds the presence of scar tissue in Covid-19 patients compelling. “For me, that’s one of the bigger take-home points,” he said. Others noted that the risk-matched group also had a large number of cardiac abnormalities, including scar tissue, so the scarring in the Covid-19 patients might not have been caused by the virus.
The German study’s corresponding author, Eike Nagel, attributed the mixed responses to the fact that “we just don’t know enough yet.” A cardiologist and expert in cardiac MRI, Nagel defended the work, pointing out that one of his measurements found scar tissue in 20 percent of those positive for SARS-CoV-2 versus just 7 percent in the risk-matched group, a nearly threefold increase. He also said he is confident that his team’s technique for measuring inflammation is accurate and meaningful because they’ve validated it in studies of other diseases. Further, the troponin levels were slightly elevated in the Covid-19 group, showing that something must be damaging the heart, he said. While it might not be severe enough to cause sudden death, he added, if the condition is chronic, it could take a toll.
Nagel is planning follow-up studies. But in the meantime, he encouraged physicians to think beyond binaries of “normal” and “abnormal” when it comes to diagnosing myocarditis. Even subtle increases in inflammation could have an effect, he said, if they persist over time.
The nuances of the myocarditis studies have been largely absent from the broader public conversation. In the month of August, the German paper was often cited in coverage of college sports. And though the OSU paper had not yet been published, its preliminary findings were shared with major athletic conferences as they deliberated about the fall season. The New York Times reported that the OSU study had already revealed an “alarmingly high rate of myocarditis” among recovered college athletes, almost all of whom had experienced mild or no Covid-19 symptoms. The article quoted the university’s director of sports cardiology, Curt Daniels: “Everybody is saying now that maybe we should do cardiac MRIs.”
Things ramped up on Sept. 3, when Penn State’s director of athletic medicine mistakenly commented in a meeting that cardiac MRI scans revealed that approximately one third of Big Ten athletes with Covid-19 had myocarditis. The university quickly issued a correction that the true rate was closer to 15 percent — but not before the national news media widely reported the wrong statistics. “This is pretty frightening,” said CNN’s Sanjay Gupta. High-profile Twitter users made similar comments: “If even young athletes in their prime come down with heart damage — there IS NO SAFE HERD (w/out vaccine) to be had,” wrote one Harvard epidemiologist.
By the end of August, even science magazines were publishing heart-related headlines that some of Undark’s sources characterize as alarmist. Among the more noteworthy headlines: “Covid-19 Can Wreck Your Heart, Even If You Haven’t Had Any Symptoms” at Scientific American and “‘Carnage’ in a Lab Dish Shows How the Coronavirus May Damage the Heart” at STAT.
“The fear has ratcheted up incredibly,” said Ackerman. After the media started reporting on Covid-19 heart problems, and again following publication of the German paper, he said worried patients started calling his clinic.
Ackerman acknowledges that there may be good non-heart reasons to delay or cancel a season: concerns about disease transmission, for instance, or lack of coronavirus testing. “But the heart cannot and should not be the driving reason.” In this context, Ackerman said, the German paper just doesn’t hold up: For one, the test subjects were older and sicker than college-athletes. Another mistake, he added, was prematurely equating the MRI scans — the significance of which are unclear — with a potentially life-threatening disease.
 |
For all of Undark’s coverage of the global Covid-19 pandemic, please visit our extensive coronavirus archive. |
Several other studies that haven’t received the same amount of attention provide another reason for restraint, said Joseph Maleszewski, a cardiac pathologist at the Mayo Clinic. The studies look at autopsies of people who died from Covid-19. And while autopsy research is still in its infancy, so far, the rate of myocarditis in the autopsies is lower than in the cardiac MRIs. Maleszewski said he worries about hasty conclusions on Covid’s effects on the heart: “If you reach that far on tenuous ground, and you wind up not being right, it undercuts the things you’re right about.” This potentially feeds the narrative that the claims around Covid-19 are mostly just politics, rather than ongoing, dynamic science, he added.
Several physicians told Undark that the overwrought messaging around myocarditis is having a ripple effect, with patients contacting their physicians to request a cardiac MRI. There are downsides to doing these tests when they aren’t warranted, said Murthy: the cost and the required resources (“In the U.S., our capacity to do these is nowhere near sufficient to test large numbers of people who have no cardiac symptoms from Covid.”) Then there’s the potential for incidental findings — things spotted on a scanner that might be causing no harm, but that fall outside the range of normal. That can start a chain of events, with a patient receiving one test after another for something that was never going to harm them, said Murthy.
And while it may seem rational to consider canceling football out of an abundance of heart-based caution, Ackerman disagreed. As director of the Windland Smith Rice Genetic Heart Rhythm Clinic, he treats hundreds of athletes, many of whom were previously disqualified from competitive sports due to preexisting heart conditions. Postponement or cancellation, he said, will have “similarly devastating consequences” on athletes’ mental wellbeing. Are we weighing all of it in the balance, he added, “or are we being selective in which item we are putting forward as the tipping point item, the playing with fire item?”
On Sept. 11, the long-awaited results of the Ohio State University study of student-athletes published in the form of a research letter in JAMA Cardiology. The authors scanned 26 college athletes who tested positive for Covid-19 and had mild to no symptoms, identifying what they termed “suspected myocarditis” in four individuals. A university press release noted that the cardiac MRI had been “effective in identifying myocardial inflammation not picked up by other methods” and that the technology has the potential to identify athletes who can safely return to play.
The motivation for the research was clinical, said Saurabh Rajpal, the lead author and a cardiologist at The Ohio State University Wexner Medical Center. It can be hard to detect subtle symptoms in athletes because they don’t get winded as easily as non-athletes, said Rajpal. So he and his colleagues decided that the best way to ensure safe participation was to include a cardiac MRI with other testing.
Unlike the German paper, the OSU study didn’t have a comparison group. That’s important to keep in mind when interpreting the results, said Kate Hanneman, a cardiac radiologist and expert in cardiac imaging at Toronto General Hospital Research Institute. Athlete hearts are different from the hearts of the general population; for example, previous studies have found scar tissue in endurance athletes. Without a point of comparison, it’s not clear whether the abnormalities spotted on the MRI scans were caused by the coronavirus. She also noted that the study participants lacked two criteria usually needed for a diagnosis of myocarditis: cardiac symptoms and elevated troponin levels.
A summary published by The American College of Cardiology made similar points, concluding: “While this study adds to emerging data, it does not imply that CMR should be performed in all Covid-19 positive patients to screen for myocardial inflammation.” A few days later, an open letter appeared online. It had been initiated by Murthy and was cosigned by roughly 50 medical professionals. Addressed to 18 medical societies, the letter asked them to discourage the use of cardiac MRIs on asymptomatic people who test positive for Covid-19.
A day after the open letter published, the Big Ten announced that football season will resume in late-October. Players who test positive for the virus will undergo comprehensive heart screening, including an MRI. Big Ten universities will create a cardiac registry, pooling the test results for future study.
Echoing others, Shenoy said he welcomes more research, and a well-designed registry could eventually provide useful data. But, he said, it’s premature to use these tests to diagnose or assess the risk for people who don’t have cardiac symptoms. “None of it,” he wrote in an email, “is supported by any evidence when it comes to asymptomatic athletes.”
Sara Talpos is a senior editor at Undark and a freelance writer whose recent work has been published in Science, Mosaic, and the Kenyon Review’s special issue on science writing.
Comments are automatically closed one year after article publication. Archived comments are below.
Boy, you guys really know how to present an in-depth report. Kind of investigation and explanation almost never seen these days, impressive.