








A Struggle to Find Adequate Care for a Common Menstrual Disorder
In 2022, Maria Stenos had her womb, ovaries, and fallopian tubes removed. For years, the 36-year-old had suffered debilitating pain and mental health issues, which appeared before the start of her period every month. “It was a last resort,” Stenos, who is now 39 and originally from California, explained, speaking from her home in Greece. She suffered from suicidal ideation: “The pain had taken away my ability to work, my ability to enjoy life.” Stenos and her partner, now husband, “got to the point with the doctor where there was no quality of life, and we were afraid that I was going to act on the ideation.”

Across the world, millions of people suffer from premenstrual dysphoric disorder, or PMDD, a condition linked with their menstrual cycle and characterized by depression and irritability severe enough to impair their daily lives. It’s unclear precisely how many women are affected by PMDD. Under the narrowest assessment, at least 1.6 percent have the disorder according to a 2024 systematic review by a group of international researchers, although the figure shifts depending on which criteria apply. (Although trans men and nonbinary people may also experience the condition, relevant data are scarce.) Other analyses suggest the figure is between 3 percent and 8 percent.
“In my experience it is probably higher due to under reporting and misdiagnosis,” wrote Nick Panay, a gynecologist and chairman of the National Association of Premenstrual Syndromes in the United Kingdom, in an email to Undark.
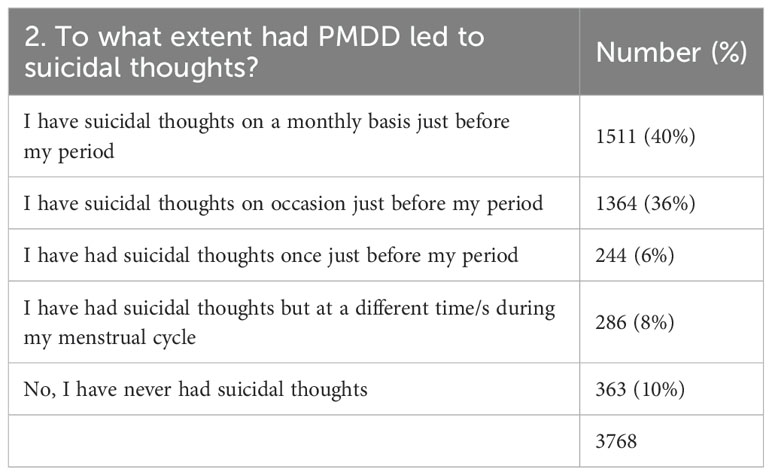
In cases like Stenos’, PMDD symptoms may be so intense as to lead to thoughts of self-harm. A 2024 U.K.-based study of more than 3,600 women with PMDD found that 82 percent had suicidal thoughts before their periods, and a quarter had tried to end their lives during what the researchers described as a “PMDD crisis.” A global survey of almost 600 women had similar findings, with 72 percent reporting active suicidal ideation at some point during their lives.
{kind=link}
{kind=link}
Doctors in the field “know just how serious it gets. People do take their lives.”
Medical bodies and doctors may vary in whether they treat PMDD as primarily a psychiatric or gynecological condition — it is, in the words of one group of clinicians, “at a crossroads between mental and gynecological health.” Treatments range from birth control, antidepressant drugs, and therapy to drug-induced menopause or surgery to remove reproductive organs.
Facing such a blurry landscape, women struggle to get the right care, and many battle for years before finding a successful treatment. Laura Murphy, like Stenos, had surgery after years struggling with her mental health. But in her experience, doctors in the field “know just how serious it gets,” she said. “People do take their lives.”
Doctors have long been aware that some women suffer from unusually harsh symptoms around their period. In 1931, a physician in New York, Robert T. Frank, noted that a subset of female patients were “handicapped by premenstrual disturbances of manifold nature.” But it wasn’t until 1987, that late luteal phase dysphoric disorder — “luteal” referring to the two-week phase before menstruation — appeared in the appendix of American psychiatry’s leading guide, the Diagnostic and Statistical Manual of Mental Disorders, then in its revised third edition. In 2013, the fifth edition — DSM-5 — moved the condition to the main text, and six years later it appeared in the 11th edition of the International Classification of Diseases, a diagnostic manual maintained by the World Health Organization.
In order to qualify for the diagnosis, patients need to experience a number of symptoms leading up to their period that cause distress or impair normal function such as irritability, hypersomnia or insomnia, and in DSM-5, “markedly depressed mood, hopelessness or self-deprecating thoughts.” DSM-5 requires at least five symptoms, and ICD-11 at least one mood symptom coupled with cognitive issues like forgetfulness.

Maria Stenos experienced debilitating symptoms, including suicidal ideation, before the start of her period every month. She saw multiple clinicians before receiving a PMDD diagnosis, and eventually had her womb, ovaries, and fallopian tubes removed.
Visual: Courtesy of Maria Stenos
“A lot of different organizations have devised criteria for PMDD, and all of them have strengths and weaknesses,” said Michael Craig, a dual-trained psychiatrist and gynecologist who co-authored the guidelines of the Royal College of Gynaecologists and Obstetricians in the U.K. When fewer symptoms are required for diagnosis, up to 80 percent of women will meet the threshold, he said, while stricter criteria bring the rate down to 5 percent. Rather than applying rigid conditions, he said he prioritizes the patient in front of him. “If you have a diagnostic system that says you’ve got to have three of one and five of the other, but they’ve only got two of one, and those two are sort of disabling their lives, it would seem foolish to say, ‘Well, you don’t reach diagnostic criteria for me to treat you.’”
Some feminist scholars worry that PMDD is a “culture-bound” phenomenon, which pathologizes healthy bodies and ignores women’s valid reactions to problems in their environment. Jessica Peters, an associate professor of psychiatry and human behavior at Brown University, disputes this characterization: “I think the only person who would suggest this is somehow over-pathologizing something is somebody who doesn’t have PMDD.”
But not all doctors are familiar with the disorder. By one estimate, 90 percent of women with PMDD are mistakenly thought to have another condition. Stenos saw multiple clinicians before receiving her diagnosis, which she eventually received from a medical herbalist in the U.K. before finding a gynecologist who took her on board. “I had been to 20 gynecologists, I had been to five or six endocrinologists, I had been entered into the pain management program in Liverpool where I was living in the U.K.,” she said. “I mean, I had gone to as many doctors as would see me, and no one had brought it up as a diagnosis. So I was diagnosed by a non-medical doctor.”
Across different countries, broadly similar approaches to treating PMDD have emerged, with variations in emphasis. In the U.S., selective serotonin reuptake inhibitors, a type of antidepressant, are a first-line therapy and the FDA has approved several for treatment of the disorder. The European Medicines Agency issued guidelines, which came into effect in 2012, citing SSRIs as a possible treatment, but has not formally approved the treatment. That may be because PMDD did not appear in the ICD-11 until 2022, as one editorial published that year suggested.
In the U.K., no licensed treatments for PMDD exist, though medical guidelines recommend SSRIs off-label. This less official manner of prescribing doesn’t make much difference in practice, but it can affect doctor “confidence and patient perceptions,” Craig wrote by email.
By one estimate, 90 percent of women with PMDD are mistakenly thought to have another condition.
When some women take SSRIs for PMDD, the drugs appear to work much more quickly than in standard treatment for depression, said Peters, who is also a clinical psychologist — a perspective backed up, albeit cautiously, by a 2024 review by Cochrane, an independent organization that assesses health research. Some women feel the impact within 24 hours of taking the drugs, said Peters, who as a psychologist does not prescribe the drugs herself. Patients describe it as being “like taking an Advil, where they can take that SSRI, and as soon as it really hits their bloodstream and it’s going through their body, they feel immediate relief.”
Patients with PMDD can take antidepressants either continually or in the two weeks leading up to menstruation. This periodic dosing can confuse people who expect SSRIs to take several weeks to work, as is standard in depression or anxiety, Craig said. In PMDD, he suggested, SSRIs may help the body process progesterone, a hormone that prepares the womb for a fertilized egg.
The Cochrane review’s latest update, which was published last year, found that when taken continuously or just two weeks before menstruation, SSRIs, were “probably effective in reducing the overall premenstrual symptoms.” (Continuous prescription of SSRIs was probably more effective, it also found.) The review authors noted that more than two thirds of recent studies had been funded by pharmaceutical companies, which could bias the findings, and that SSRIs could have “unwanted effects, with the most common being nausea, a lack of energy and sleepiness.”
Oral contraceptives are another early treatment, although Peters cautioned that in some women they can also cause depressive symptoms and other side effects. Doctors will often prescribe a hormonal contraceptive as a first-line treatment, “which we don’t recommend,” said Peters, who is on the clinical advisory board of the International Association for Premenstrual Disorders, or IAPMD.
But some European countries are hesitant about SSRIs, Craig said. Jeppe Schroll, a Danish gynecologist and one of the Cochrane review’s co-authors who has worked on guidelines for the WHO, said he is fairly certain that SSRIs decrease PMDD symptoms, but that doctors should only discuss them with patients when other options, like hormonal contraceptives, have failed. Danish physicians, he said, are generally wary of them. “It seems that SSRIs are pretty difficult to discontinue and that they will sometimes give some withdrawal effects,” he added. “And that’s something that we are pretty concerned about, at least in Denmark.”
When some women take SSRIs for PMDD, the drugs appear to work much more quickly than in standard treatment for depression.
If the symptoms persist, patients may go on drugs that suppress hormones by switching off ovarian function. These medications, known as GnRH agonists, induce chemical menopause; one common brand name is Lupron. The side effects of chemical menopause can be severe, including bone density loss and risks to the heart. To fend off menopausal symptoms, doctors prescribe estrogen — but this triggers a further cascade, Craig said. “The problem is you can’t just leave somebody in that state,” he said, adding, “you have to give them progestogens at some point, because if you don’t, the inner lining of the womb starts to get thicker, and you could have an increased risk of endometrial cancer.”
Samara Steinmetz, 22, from Chicago started noticing symptoms of PMDD after hospitalization following a car accident. She said she had always been “kind of bitchy” before her period, but began to experience peaks of rage and sleep deprivation in the 10 days leading up to menstruation. Steinmetz first tried birth control pills. “They helped more than any antidepressant I was on,” she said.
But each contraceptive only worked for a while. After testing out six types, Steinmetz raised the possibility of surgery with her doctor. “She was like, ‘Well, slow down, cowboy,’” she recalled. “She’s like, ‘I do hear you, this other stuff that we’ve tried hasn’t worked. We should explore more options.’ So she put me on the Lupron.”

For this condition, her insurer, Medicaid, did not cover Lupron, which is licensed to treat endometriosis, uterine fibroids, prostate cancer, and precocious puberty, but the manufacturer offered her eleven months’ treatment on a charitable basis. It took a while to adjust, Steinmetz said, and she began to feel pain in her bones and vaginal itching. Her gynecologist said she had vaginal atrophy and prescribed an estrogen cream for it, alongside other hormone-based treatments to reduce menopausal symptoms. Once her system got used to the regimen, it was blissful, she said, but she can still have side effects: During a holiday with her partner and his family after a recent increase in her hormone dosage, her estrogen levels went too high, she recalled in an interview. “I was freezing cold, but I was sweating super hard. I was shaking. My pupils were huge, and I had the worst pit of anxiety I’ve ever experienced.”
After removing the estrogen patch, she felt better, and once her access to Lupron runs out, she wants surgery. “I’ve been given a taste of what my adult life can be without this awful disorder and now I’m so scared to have to go back,” she wrote to Undark in an earlier interview via direct messaging on Reddit.
She said that she doesn’t expect surgery to be much different than being on Lupron, “except being assured that my PMDD won’t ever come back.”
The number of women who have surgery, though small, is still notable. Craig, who tends to see more severe patients in his practice at the National Female Hormone Clinic in London, described it as “not a tiny percentage.” His team has not formally assessed the number of patients who have their ovaries and womb removed, he said, “but I would guess that it’s about one in 35, 40.”
But doctors shy away from carrying out these procedures, according to Jeppe Schroll and some of the women Undark interviewed who had sought them out. Removing ovaries or other organs from an otherwise healthy patient is “something that we are usually quite hesitant about,” said Schroll. He has never performed such a procedure himself but knows of patients who have been happy with the result. Still, he said, “most doctors will find it a little bit challenging to do this type of surgery.”
“I agree it’s a fairly rudimentary treatment for something that could be more nuanced, but it isn’t yet.”
Jayashri Kulkarni, a psychiatrist and director of the HER Centre at Monash University in Australia, went further, describing surgical treatment for PMDD in most cases as “dreadful!” Kulkarni has co-published a study that found that women with PMDD were more likely than others to have experienced childhood trauma, and she and her co-authors hypothesized that stress affected their hormonal system. Over email, she wrote, “I think it is a very ‘concrete’ approach to PMDD by non-understanding clinicians, perhaps a hangover from the days of ‘hysteria and the wandering womb’???” — referencing ancient Greek theories of female madness and disease originating in the reproductive organs. She continued: “Old fashioned gynaecologists tend to operate in these situations as per old training.”

Laura Murphy had surgery after years of struggling with PMDD. “I think a lot of people think that surgery is kind of like a go-to for PMDD, and it’s really not, you know? It’s the end of the line,” Murphy said.
Visual: Courtesy of Laura Murphy
Craig said he understood these concerns but said that for some women, surgery is the only option since no other treatment exists: “I agree it’s a fairly rudimentary treatment for something that could be more nuanced, but it isn’t yet.”
But both Stenos and Murphy told Undark of the positive impact surgery had on their lives. Murphy had it when she was 37 after years of debilitating panic attacks and depression. Despite having her ovaries, tubes, and womb removed, she still experiences cyclical symptoms like anxiety. Last year, Murphy had a follow-up procedure to remove ovarian remnants, which she thought could be releasing hormones.
The risk of ovarian remnants is less than one percent, said Panay. A minority of women have ongoing symptoms after the procedure, he said, perhaps due to hormonal fluctuations triggered by HRT or residual cyclical changes in the brain; but more research is needed, he said.
After the surgery, Murphy said she felt relief, but recovery has been complicated. “It is a serious operation,” she said. “I think a lot of people think that surgery is kind of like a go-to for PMDD, and it’s really not, you know? It’s the end of the line. It’s when you’ve tried everything else.”
Considering the number of people affected by PMDD, funding is disproportionally low in the U.S., according to Liisa Hantsoo, an assistant professor in the department of psychiatry and behavioral sciences at Johns Hopkins School of Medicine. (She also sits on the clinical advisory board of the IAPMD with Peters.) Last year, Hantsoo co-authored a commentary analyzing NIH funding in the Journal of Women’s Health. Assuming that 3 percent of women have PMDD — which she described as a conservative estimate — would mean it affects more than two million women in the U.S., compared with postpartum depression, which impacts just over 440,000, or about 12 percent of births. Yet postpartum depression received 15 times more grants.
At conferences on women’s mental health, Hantsoo said, postpartum depression is often a significant focus, while PMDD rarely features. “I think PMDD should get way more attention than it does, again, just because so many more people are affected by it.”
Considering the number of people affected by PMDD, funding is disproportionally low in the U.S.
The women Undark spoke to encouraged others to advocate for themselves. Maria Stenos wrote by email that for her, surgery was “completely life changing.” She told Undark that, “the PMDD symptoms went away as soon as I woke up, they never came back.”
She sometimes gets hot flashes and other menopausal symptoms, but compared with the pelvic pain and suicidality she had before her periods, it’s a relatively easy burden. Stenos wants other women to know about PMDD, and said she believes in advocacy about “gynecological issues, especially something like this that a lot of people don’t fully understand.”
She added, “You can feel crazy when you have it, especially when the doctors tell you that there’s nothing wrong.”
If you or someone you know are in crisis, please call the National Suicide Prevention Lifeline at 1-800-273-TALK (8255), or contact the Crisis Text Line by texting TALK to 741741.