








Do Masks Work? It’s a Question of Physics, Biology, and Behavior.
On March 28, 2020, as Covid-19 cases began to shut down public life in much of the United States, then-Surgeon General Jerome Adams issued an advisory on Twitter: The general public should not wear masks. “There is scant or conflicting evidence they benefit individual wearers in a meaningful way,” he wrote.
Adams’ advice was in line with messages from other U.S. officials and the World Health Organization. Days later, though, U.S. public health leaders shifted course. Mask-wearing was soon a pandemic-control strategy worldwide, but whether this strategy succeeded is now a matter of heated debate — particularly after a major new analysis, released in January, seemed to conclude that masks remain an unproven strategy for curbing transmission of Covid-19 and other respiratory viruses.
“There’s still no evidence that masks are effective during a pandemic,” the study’s lead author, physician and epidemiologist Tom Jefferson, recently told an interviewer.
Many public health experts vigorously disagree with that claim, but the study has caught attention, in part, because of its pedigree: It was published by Cochrane, a not-for-profit that aims to bring rigorous scientific evidence more squarely into the practice of medicine. The group’s highly regarded systematic reviews affect clinical practice worldwide. “It’s really our gold standard for evidence-based medicine,” said Jeanne Noble, a physician and associate professor of emergency medicine at the University of California, San Francisco. One epidemiologist described Cochrane as “the Bible.”
The new review, “Physical interventions to interrupt or reduce the spread of respiratory viruses,” is an updated version of a paper published in the fall of 2020. It dropped at a time when debates over Covid-19 are still simmering among scientists, politicians, and the broader public.
For some, the Cochrane review provided vindication. “Mask mandates were a bust,” conservative columnist Bret Stephens wrote in The New York Times last week. “Those skeptics who were furiously mocked as cranks and occasionally censored as ‘misinformers’ for opposing mandates were right.”
Meanwhile, masks continue to be recommended by the U.S. Centers for Disease Control and Prevention, which describes them as “a critical public health tool.” And this winter, some school districts issued short-term mandates in an effort to curb not just Covid-19, but other respiratory viruses, including influenza and RSV.
The polarized debate conceals a murkier picture. Whether or not masks “work” is a multilayered question — one involving a mix of physics, infectious disease biology, and human behavior. Many scientists and physicians say the Cochrane review’s findings were, in a strict sense, correct: High-quality studies known as randomized controlled trials, or RCTs, don’t typically show much benefit for mask wearers.
But whether that means masks don’t work is a tougher question — one that has revealed sharp divisions among public health researchers.
The principle behind masks is straightforward: If viruses like SAR-CoV-2 or influenza can spread when droplets or larger particles travel from one person’s nose and mouth into another person’s nose and mouth, then putting up a barrier may slow the spread. And there’s certainly evidence that surgical masks can block some relatively large respiratory droplets.
Early in the pandemic, though, some researchers saw evidence that SARS-CoV-2 was spreading via tinier particles, which can linger in the air and better slip around or through surgical and cloth masks. “Sweeping mask recommendations — as many have proposed — will not reduce SARS-CoV-2 transmission,” respiratory protection experts Lisa Brosseau and Margaret Sietsema wrote in an April 2020 article for the Center for Infectious Disease Research and Policy at the University of Minnesota.
Their colleague Michael Osterholm, a prominent epidemiologist, was more blunt: “Never before in my 45-year career have I seen such a far-reaching public recommendation issued by any governmental agency without a single source of data or information to support it,” he said on a podcast that June. (The Minnesota center receives funding from 3M, which manufacturers both surgical masks and respirators.)
In a recent interview with Undark, Brosseau stressed that she thinks cloth and surgical masks have some protective benefit. But she and others, including Osterholm, have urged policymakers to emphasize tight-fitting respirators like N95s, rather than looser-fitting cloth and surgical masks. That’s because there’s clear evidence that respirators can effectively ensnare those tiny particles. “A well-fitting, good quality respirator will trap the virus, almost all of it, and will greatly reduce your exposure to it,” said Linsey Marr, an engineering professor at Virginia Tech who studies the airborne transmission of viruses.
When air flows through a respirator, it passes through a dense mesh of fibers. Those tiny particles collide with the fibers and get stuck, thanks to electrostatic forces — the same force that makes hair stick to a balloon.
There is “a huge reduction in the number of particles that get through,” Marr said. (Indeed, the “95” in the N95 rating indicates that a mask, used properly and under the right conditions, is designed to capture roughly 95 percent of airborne particles.)
A popular online physics education channel offers an animated breakdown of how N95 masks work to reduce exposure to airborne particles.
In the laboratory, researchers can actually test out respirator performance. For one paper, published in 2020, scientists placed two mannequin heads in a translucent box. Using a nebulizer and actual SARS-CoV-2 virus, they piped “a mist of virus suspension” through the mouth of one mannequin, mimicking an exhaling person. They used a ventilator to draw air into the other mannequin’s mouth. Finally, they fitted the mannequins with various combinations of masks, respirators, or nothing at all, and tested how much of the virus evaded capture as it journeyed between the mannequins. Cloth and surgical masks did have an effect — but were substantially outperformed by the N95s, which captured most of the viral particles.
Just because an N95 captures particles in the lab, however, doesn’t necessarily mean it will stop an actual person from getting infected out in the world. Part of the issue is that people don’t always wear respirators properly. And, even if the respirator performs well, the viral particles that slip through could be enough to make a person sick anyway. In the mannequin study, even an N95 taped snugly to a mannequin’s face failed to capture all the particles.
Over the past 15 years, a handful of research teams have tried to test out mask and respirator performance in the real world, through randomized controlled trials. Such studies are often considered the highest standard of evidence, because they can minimize sources of bias. In one such study, conducted in the winter of 2009 and 2010, the Australian epidemiologist Raina MacIntyre and several colleagues divided nearly 1,700 health care workers in Beijing into three groups. People in one group were told to wear surgical masks at work. Another group was instructed to wear an N95 at all times. And a third group was asked to wear an N95 only during certain high-risk procedures. Then, for four weeks, the team tracked how often the participants got sick.
MacIntyre and her colleagues reported that the people who wore N95s all day were significantly less likely to develop a respiratory illness than everyone else.
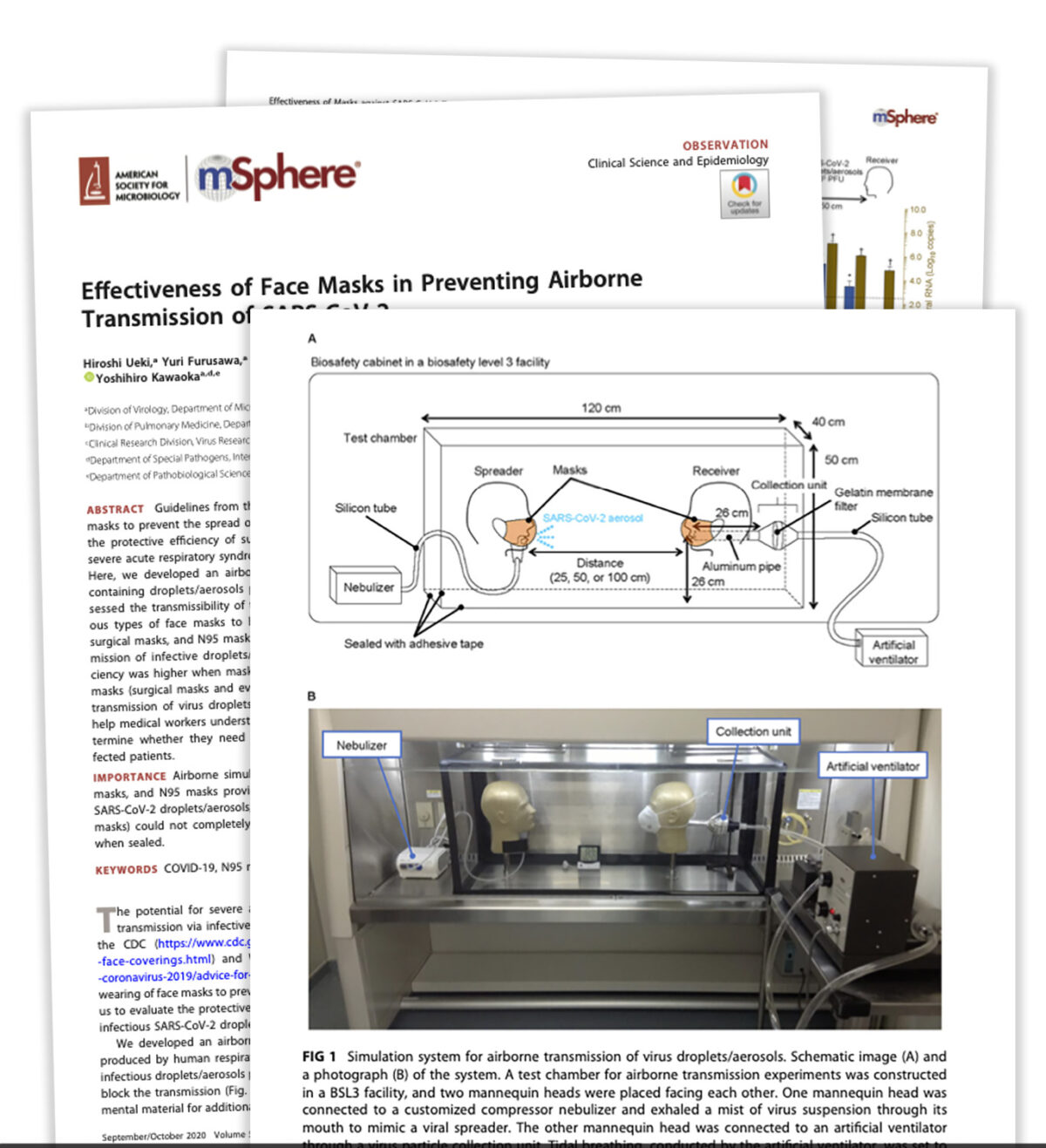
One 2020 study using mannequin heads found that cloth and surgical masks did have an effect — but were substantially outperformed by the N95s, which captured most of the viral particles.
Other studies have produced mixed results. Some found that the masks or respirators had a small effect on someone’s odds of getting sick, but not always enough to be considered statistically significant. Others didn’t find any benefit at all when comparing N95s to surgical masks, or even surgical masks to non-masking.
Do those findings apply, though, when millions of people are masking together, in the middle of a pandemic? At this scale, the question of whether or not masks work can be treated as a policy question: Did mask requirements actually reduce the spread of Covid-19? But doing a randomized controlled trial to answer this question is probably impossible, said Jing Huang, a biostatistician at the University of Pennsylvania’s Perelman School of Medicine. It’s not easy to just ask a few dozen randomly selected cities to implement mandates, and a few dozen to avoid mandates, and then track what happens.
And yet, this scenario did happen naturally during the Covid-19 pandemic: Some places put in mask mandates, and others did not. This sort of natural experiment opened up an opportunity for researchers to sift through health data in these different locations and try to suss out patterns — and Huang and her colleagues recently did just that. They matched 351 counties in the United States that had implemented mask mandates with counties that did not have a mandate, but that were otherwise similar in several other respects. This means that, when possible, the Covid rates in a Republican-leaning, suburban county in the South that implemented a mask mandate during moderate Covid-19 spread would be measured against infection rates in another right-leaning, suburban Southern county that did not put a mandate into place at the same time.
Huang’s analysis found that mask mandates were associated with substantially dampened Covid-19 spikes, although the benefit waned over time in some counties. The reason behind that waning was unclear, but could perhaps be could be due to fatigue with the mandates, the researchers suggested. Similar studies have often — but not always — found a positive effect.
Whether the masks were responsible for those benefits, though, was hard to pin down, Huang said. It’s possible that other factors — such as other policies implemented alongside mask mandates, or greater social distancing — actually kept Covid-19 rates lower, rather than the masks themselves. “I think it’s very difficult,” Huang said, “to make a causation conclusion.”
The CDC has cited other observational studies to justify its masking recommendation. One 2022 study found that people in California who chose to wear N95s were less likely to catch Covid-19 than people using other kinds of respiratory protection, who were themselves less likely to fall ill than people did not wear a mask at all. But the study was criticized for doing little to control for all the other ways people who wear N95s may behave differently than people who never wear masks. Was it the masks that made the difference? Or was it those other cautionary behaviors that people who tend to wear N95s also engage in that reduced their risk?
Cochrane’s methods were designed precisely to unravel these kinds of vexing medical questions. The organization was launched in 1993, with the mission, as reporter Daniel Kolitz wrote in a feature for Undark, of “gathering and summarizing the strongest available evidence across virtually every field of medicine, with the aim of allowing clinicians to make informed choices about treatment.”
Today, Cochrane maintains a network of thousands of affiliated researchers, who produce hundreds of reviews each year while working under the Cochrane banner. Those reviews tend to answer very specific questions: For example, does taking vitamin C reduce “the incidence, the duration or severity of the common cold”? Each team first searches the vast scientific literature, trying to amass an exhaustive list of relevant published and unpublished studies. Then, they select studies that meet Cochrane’s thresholds for rigor, and systematically organize and synthesize the data, aiming to produce a succinct answer to the original question.
Those reviews prioritize randomized controlled trials — things like the experiment with the Beijing health care workers — over other kinds of studies.
Tom Jefferson, who is an instructor in the Department for Continuing Education at the University of Oxford, is the first author on Cochrane’s recent masking review. For nearly two decades, he’s been part of a Cochrane team that examines the effects of certain interventions on the spread of respiratory viruses. The team has considered a range of questions: Do respirators help slow the spread of respiratory illnesses? Does handwashing? Does gargling?
Jefferson’s group published their first systematic review of these kinds of questions in 2006. For the most recent, updated review, Jefferson and 11 collaborators synthesized evidence from 78 such RCTs, including 18 studies that specifically examined mask and respirator use. (They also looked at five ongoing studies, including two that look at mask use.) Their conclusion is principally about the absence of evidence: Taken together, they found, those studies simply do not offer evidence that asking people to wear an N95 instead of a surgical mask significantly reduces their odds of getting sick. Similarly, they did not find evidence that wearing surgical masks offered an advantage over wearing nothing at all.
Few of the studies took place during the Covid-19 pandemic, instead looking at infections during cold and flu seasons. And the majority of the studies only looked at whether masks and respirators protect the wearer from getting sick — not whether they reduce the odds that a sick mask-wearer will infect other people.
Some researchers agree that randomized controlled trials don’t currently show clear-cut evidence that masks and respirators reduce the wearer’s odds of getting sick. But, they argue, RCTs may not actually be the best source of evidence for determining whether masks confer protection. “Strictly speaking, they’re correct that there’s no statistically significant effect,” said Ben Cowling, an epidemiologist at the University of Hong Kong whose research is cited in the Cochrane review. “But when you look at the totality of evidence, I think there’s a pretty good indication that masks can protect people when they wear them.”
In particular, Cowling said, mechanistic studies — like those conducted with mannequins — do offer strong evidence that respirators cut down on the passage of viral particles.
Huang, the Penn biostatistician, is among others who argue that, in many RCTs examining mask use, the sample sizes are just too small. Even if masks are effective, that may not show up as a statistically meaningful result. “When the effect is moderate, or small, we really need a large sample size to find a significant difference,” said Huang. Many of these RCTs, she said, simply weren’t large enough to find some potentially meaningful signal.
And even if the effect is modest, during peak periods of a pandemic, small advantages can have a large impact by reducing the number of sick patients seeking hospital care at the same time. “From a public health perspective,” said Cowling, “reducing the reproductive number by even 10 percent could be valuable.”
For a complex issue like masks, Trish Greenhalgh is among other researchers who suggest that an RCT may be an imperfect tool. “I’m not against RCTs,” said Greenhalgh, a physician and health researcher at the University of Oxford. “But they were never designed to look at complex social interventions.”
Greenhalgh is an influential figure in the evidence-based medicine movement — her book “How to Read a Paper: The Basics of Evidence-Based Medicine and Healthcare” is in its sixth edition — but she has at times been critical of what she characterizes as an overreliance on RCTs. Greenhalgh characterized some of her colleagues as, in effect, RCT hardliners — focused on RCTs at the expense of considering other kinds of evidence. In that mindset, she said, “it seems that an RCT, however bad, is better than an observational study, however good.”
Cochrane’s own leadership seems to share some of those concerns. In November 2020, when Jefferson’s team published an earlier version of their review, Cochrane published an accompanying editorial, warning policymakers to move cautiously with the results, and not to interpret them as definitive evidence that masks and respirators don’t work. Instead, the group wrote, “there may never be strong evidence regarding the effectiveness of individual behavioral measures.”
Some observers have suggested that such warnings are more about politics than science.
In an interview with the journalist Maryanne Demasi, Jefferson accused Cochrane of slow-walking an earlier version of the review, and of writing the editorial in order “to undermine our work.” In an email sent to Undark via Harry Dayantis, a Cochrane spokesperson, the editor in chief of the Cochrane Library, Karla Soares-Weiser, said the processing time was standard for such a long review. “We wrote the editorial to help contextualize the review in the hope that it would help to prevent misinterpretations of the findings,” she wrote. “As we’ve seen from the response to the 2023 update, the risk of misinterpretation is very real!”
[ UPDATE: A week after publication of this article, Soares-Weiser posted a statement on the Cochrane Library website indicating that the review’s plain-language summary and abstract were being revised to address these sorts of misinterpretations. ]
The review is not the first time that Jefferson has found himself challenging prevailing medical opinion. Years ago, he drew attention for arguing that the benefits of influenza vaccines had been overstated. (A 2009 article in The Atlantic described him as “the most vocal — and undoubtedly most vexing — critic of the gospel of flu vaccine,” noting that he had become “something of a pariah” among flu researchers.) He has spent years arguing that the drug oseltamivir, also known as Tamiflu, and another antiviral medication may be less beneficial for influenza patients than drugmakers and public health authorities have claimed. More recently, he and another author on the Cochrane review, Canadian physician and World Health Organization adviser John Conly, have questioned the role of small airborne particles in transmitting SARS-CoV-2.
Jefferson has also done some writing for The Brownstone Institute. Founded by libertarian Jeffrey Tucker, the organization is broadly opposed to public health restrictions during the Covid-19 pandemic.
Jefferson declined to be interviewed for this article, sharing links to three Substack posts in which he criticizes press coverage of the Covid-19 pandemic. “Most media are as complicit in spreading fear and panic as governments and their psyops people,” he writes in one of the posts, going on to draw an analogy between reporters and Nazi functionaries.
Attempts to arrange interviews with four other authors of the Cochrane review, including Conly, were unsuccessful.
At times, the conversation about masks can verge on larger questions about human nature, and about how research should take into account the messiness of people’s behavior.
At issue is a contentious detail: In many of the RCTs analyzed in the Cochrane review, it’s not clear whether the people who were told to wear masks or respirators actually did so consistently and correctly. In addition, many such studies only ask people to wear respiratory protection for part of the day, meaning even if the mask or respirator works to stop infections when it’s on, the wearer may just get sick at other times. Marr, the Virginia Tech professor, compared this to a study that asks people to wear condoms only half the time they have sex: “What do you think’s going to happen?”

Some people are skeptical that such distinctions really matter, at least when it comes to policymaking. “Your policy has to exist in the real world. That’s the thing,” said Shira Doron, a physician and the chief infection control officer at Tufts Medicine. A respirator, used perfectly and continuously, may work to reduce the spread of Covid-19. But if there’s a public health intervention that requires strict adherence, and almost nobody seems willing or able to follow it, is that actually an effective intervention at all? What does it even mean to say that it works?
Noble, the emergency physician, has led the UCSF Hospital emergency department’s Covid-19 response. Perfect masking, she said, is out of reach for many people. In some cases — she brought up elderly patients who struggle to communicate when masked — it can even have harms. And masking policies, she said, don’t always seem to recognize that reality, especially at a stage in the pandemic when vaccines are widely available. Her own work suggests that even fitted respirators, worn by health care workers, can swiftly lose their shape and fit, perhaps undercutting their protective benefits. “It’s just harder to fit a human being than it is a mannequin,” she said. “And then we just cannot wear them correctly, for any length of time, because of the discomfort.”
Doron spoke warmly about the Cochrane review, while stressing that it had limits. “This study has concluded, not that masks don’t work, but that there is not evidence that masking on a population level decreases the incidence of infection. That’s what it proves,” she said. She still thinks a good, well-fitting respirator can help prevent someone from catching Covid-19. “Why do I think that I think that? Because of the totality of evidence from non-RCTs that address that question. But do I know it? No, I do not.”
It can be difficult to determine what all of this evidence — and gaps in evidence — mean for mask mandates. Cowling spoke with Undark via Skype from Hong Kong, where officials continued to enforce a mask mandate until this week, issuing steep fines for people who did not cover up in public spaces, both indoors and outdoors.
Cowling, who heads the Department of Epidemiology and Biostatistics at the University of Hong Kong’s School of Public Health, expressed doubts about that kind of policy. He argued that the evidence is clear that widespread masking, deployed during a pandemic surge, may help to flatten the curve and save lives. “That’s the exact scenario that public health measures are designed for,” he said. But “that’s not the way they’ve been used in the last years,” he added.
“What’s happened in many parts of the world is that measures are brought in and kept in place,” Cowling said, “far longer than they’re needed.”
Comments are automatically closed one year after article publication. Archived comments are below.
no they don’t work to stop the spread of any airborne virus, period. There is no conflicting evidence, because there can not be any to prove it stops anything, except by those who wish to cherry pick data and manipulate factual evidence. You have to be some kind of special to believe they stop the spread of anything.
You boot licking leftists crack me up. Wear you masks idiots. That way we can all laugh at you.
What does the “N” in and “N95” mask mean?
It means that mask is effective against non-oil particles, correct?
So why are we recommending an N95 mask to protect against the Covid19 virus, which is enveloped in a lipid layer?
No. They don’t. When 78 studies including 3 giant RCTs find “no conclusive evidence that community masking as an NPI made a difference”, it’s time to stop asking this inane question and accept that masks are useless. Even N95s.
Regardless of these pro and con discussions, I personally believe that masks, when properly used, prevented the spread of Covid. When Covid hit my hospital, it was all hands on deck. Before we were assigned to Covid Care, we spent a day being instructed in all safety measures related to infection, proper techniques for PPE dressing and undressing (hate donn and doff). Proper mask technique was crucial. In almost 3 years, I have never contracted Covid. I am also fully vaccinated. I have only recently begun to relax mask wearing as things have greatly improved.
yes they do
When properly worn, unlike the guy wearing mask with his nose exposed shown as he is inhaling the air…
OhMyGOD! I have to wear a mask? What an incredible imposition! It’s almost as bad as having to walk on my knees. No, it’s worse. It’s taking away my God given freedom. The fact that it might stop someone from getting covid is completely irrelevant. Anyone making those suggestion should be hung drawn and quartered. GROW UP!
https://thenationalpulse.com/2022/05/26/counties-with-mask-mandates-had-higher-covid-19-death-rates/
https://thenationalpulse.com/2022/05/16/study-finds-correlation-between-mask-compliance-and-covid-deaths/
https://www.theblaze.com/op-ed/horowitz-nail-coffin-mask-religion
we cannot live without dirt
I think this is great perspective. I have a question. Is it likely that in any of the trials, they could have statistically found a 5-10% difference in transmission (arbitrary choice–the point is low percentage benefit). If there were such a modest difference, but the ability to power a study enough to detect it was totally impractical, would we still conclude the use was not worthwhile? When dealing with large numbers of people, as in public health, even small amounts of benefit often translate to a large number. What percentage reduction is not meaningful, or worth the effort, and who decides?
Simple. The numbers you are stating, even if they existed, are irrationally low for any mandate. Who decides? The individual does. To engage a government mandate on covering faces (think burkas), shouldn’t there be a significant cause for such an overt act by government which itself has proven drawbacks?
I edited a paper that was written during the pandemic’s first year. It looked at the numbers of new cases, the numbers of hospitalizations, and the numbers of deaths in different states through time. In several states, reductions in each of those numbers followed the advent of mask mandates by a certain number of days. That number of days varied only slightly from state to state. (The authors did not get the paper published because they felt that events had rendered the paper obsolete by the time they were ready to publish. In light of this new mask controversy they are thinking agin of publishing.
This is basically cherry-picking the straw-manned MEDIA use of a VERY questionable study, that libertarian think-tanks picked-together from whatever conformed with their tropes (to pack aerosol-spread unmitigated schools, workplaces, BARS, planes, clubs, houses-of-worship, dentist & medical offices & restaurants with sneeringly brainwashed mouthbteathers to fill pockets. Social networking advocacy PR solution firm paid sophistry is NOT science! Sort of like your “Why are fools AFRAID of Fracking, decaying fission reactors, PhARMA monopolies, bomb trains, herbicide crop dessication & picking wars to save planet destroying fracking Ponzi scheme.
Right on, bro!