






When ‘Concierge Medicine’ Came to Town, I Had Some Questions. I Still Do.
Earlier this year, the health system at the University of Michigan in Ann Arbor became the latest to roll out a “concierge medicine” program, joining the ranks of other prominent academic health centers, including Duke Health, Stanford Health Care, and Partners HealthCare, which is affiliated with Harvard Medical School.
VIEWPOINTS
Partner content, op-eds, and Undark editorials.
If you’re like me circa five months ago, you may not know what “concierge medicine” is (hint: It doesn’t involve getting an MRI in the lobby of a Four Seasons). Such programs, I’ve since learned, grew out of the private, for-profit sector, and they have traditionally had a fairly straightforward, market-driven mission: For a lot more money — sometimes as much as $80,000 annually per family — you can purchase a lot more personalized health care attention than you would get from a typical insurance plan. The migration of concierge medicine into academic health care settings is a newer thing, and while the fees are far less mercenary — I found programs online ranging anywhere from $2,500 to $6,000 per person in annual fees, on average, plus the cost of traditional insurance — they offer subscribers similar benefits: Access to a primary care physician at any time of day or night, unhurried appointments, and specialty care coordination.
To some, the whole concierge medicine concept — in any context — sounds like a revolutionary model of health care delivery that enhances the doctor-patient relationship. To others, it looks like an elitist program whereby scarce medical resources are siphoned off from the vast majority of patients and delivered to the wealthy. Those divergent views can become even more pointed in an academic health care setting, where backers position concierge medicine not just as a fast-lane for campus power brokers, but as a beneficent money maker — one that allows academic health centers to play Robin Hood by using concierge philanthropy and fees to fund the rest of the health system, including care for poor patients.
That all sounds great, but when concierge medicine first came to my campus, I had some basic questions: Is such a system fair and ethical? Do its luxury aspirations belong at my public alma mater, which recently renewed its commitment to diversity, equity, and inclusion? And most importantly, as a science writer, I wondered what sort of empirical evidence exists to show that concierge programs provide any benefit to anyone, rich or poor?
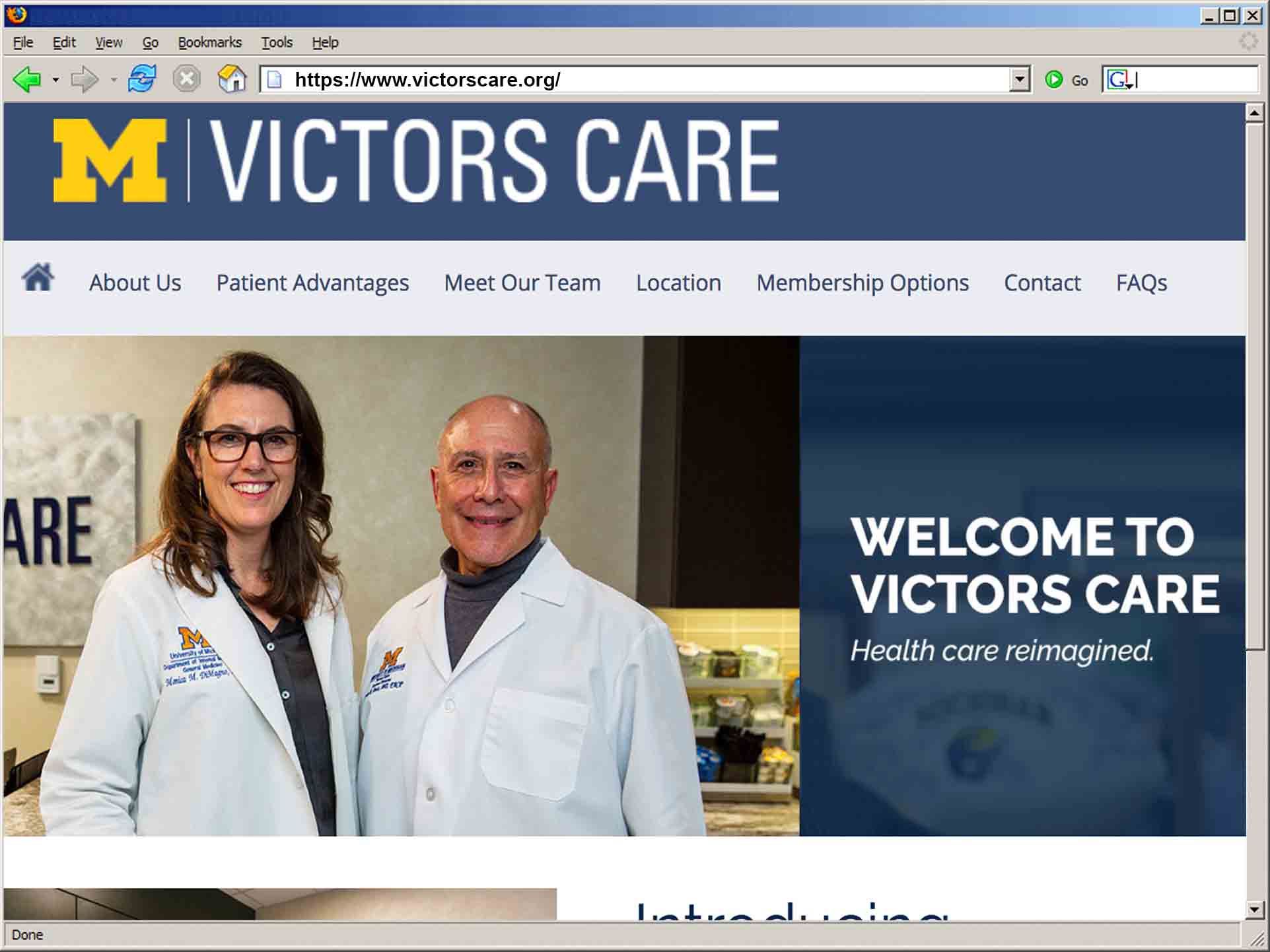
I first became aware of the program in early 2018. This was several weeks after the university health system, Michigan Medicine, mailed invitations to select donors announcing the Victors Care program — its name a nod to the university’s fight song. With the slogan “Health Care Reimagined,” the invitation promised members “an unprecedented level of access, convenience, and individually tailored support.”
In leafy Ann Arbor, Victors Care went down like a Styrofoam cup at a zero-waste party.
A January 29 letter to the health system administration, now signed by more than 300 faculty members from 16 departments, outlined an array of concerns. The Michigan Nurses Association, expressed their disapproval, too: “Nurses … are speaking out with concerns that this program is a move towards separate and unequal health care,” they wrote in a February press release. And in March, more than 100 medical residents and fellows issued their own letter, arguing that programs like Victors Care “cater to the privileged and threaten to widen the health disparities gap that so many of us entered into medicine to help narrow.”
These arguments reflect pressing health care concerns across the United States, which has a well-documented health care gap that falls along socioeconomic lines. In 1980, a wealthy 50-year-old man could expect to live 5.1 years longer than a similarly aged poor man. Thirty years later, that difference had more than doubled to 12 years. Further, from 2000 to 2014, the number of seniors reporting good health increased by 21 percent among non-Hispanic whites. During that same period, the number of black seniors reporting good health decreased by 17 percent.
One might assume that given their relatively worse health, poor Americans would account for a higher proportion of health care spending. While this was true for the decades following the creation of Medicare and Medicaid in 1965, things began to change in 2004, when per capita health care spending for the poorest 20 percent of Americans fell annually for 8 straight years. At the same time, per capita health care spending for the wealthiest 20 percent was rising. By 2012, spending for the wealthiest 20 percent of Americans exceeded that of the other groups.
And then, of course, there’s the waiting. According to a 2017 survey of 30 regions across the U.S., people in large metropolitan markets can expect to wait an average of 24 days for a new patient appointment, 30 percent longer than in 2014. Break the data down further and things look even worse: In Boston, the average new patient appointment with a family medicine physician requires waiting 109 days. Not great, but better than Albany, New York, where the average wait is just over four months.
The survey didn’t include Ann Arbor, but I assure you, we’ve got long lines here, too — and I’m not just referring to traffic jams on football Saturdays. “Some sub-specialties, [such as] endocrinology and neurology, have traditionally been impossible” to get into, says Joel Greenson, a pathologist at Michigan Medicine. He knows from personal experience. When he suffered a bout of back pain, he waited three months for an appointment for an epidural injection. And it’s not just sub-specialties. In mid-June, I scheduled an appointment with my primary care physician. Her next available appointment was September 10 — a mere 13 weeks away.
This, too, is a problem that concierge medicine promises to fix — for a price. Like several physicians I spoke with, Greenson learned about Victors Care when he received the invitation to sign up as a patient. He went to the Victors Care website (which has been revised in light of the blowback) and noticed that the program promised to assist patients with specialist appointments.
“Does that put them at the front of the line for these things?” Greenson wondered. “Because if it does, then that’s just wrong.”
Concierge medicine — sometimes referred to as “luxury” or “retainer” medicine — is not a new approach to delivering health care. The former team doctor for the Seattle Supersonics founded the first concierge clinic in 1996. Four years later, Virginia Mason Health System in Seattle opened the country’s first hospital-based concierge medicine program, and in 2004, Tufts Medical Center opened what is believed to be the first “general internal medicine retainer practice embedded within the structure of an [academic health center,]” according to a 2010 Academic Medicine article.
As far as I can tell, exact numbers are not available, but a host of academic health centers have followed suit, including UNC Health Care, under the helm of Dr. Marschall Runge, who came to Michigan Medicine in 2015 and now serves as executive vice president for medical affairs and medical school dean.
If staff at any of these other academic health centers revolted, I can find no record of it, but on February 28, at the request of University of Michigan faculty, a panel discussion was convened at University Hospital to discuss the ethics of Victors Care. At the outset, Runge explained the program’s various justifications — including an insistence that patients had expressed interest in it. But the real mic drop came when Runge said that Victors Care is designed “to bring U-M supporters … into our system in a way that they will learn more about health care and they will donate toward health care for people not as fortunate as they are.”
A panel discussion at the University of Michigan grappled with the ethics of Victors Care. Some of the explanations offered by staff didn’t immediately make sense.
That reasoning initially struck me as odd, given that the proportion of uninsured adults has fallen dramatically across the country as a result of the Affordable Care Act. Here in the Wolverine State, 16 percent of adults lacked insurance in 2013. Three years later, that number was 8 percent.
Nevertheless, if, like me, you care about Michigan Medicine because of its social mission — teaching, research, and caring for vulnerable populations; because you met your husband during his first year of medical school in Ann Arbor; because you gave birth at Michigan Medicine twice; and you once brought your son to the ER, where he was swiftly diagnosed and received emergency surgery for a potentially life threatening-condition. If you’re like me, then the possibility of providing better care to vulnerable populations is worth pursuing — perhaps even if it means creating a health care fast-lane for the rich.
Other health systems, after all, do use concierge funds to cross-subsidize their endeavors. For example, in the 2010 Academic Medicine article, a team from Tufts Medical Center outlined how Tufts’ concierge program cross-subsidizes the Division of General Medicine, using surplus funds to promote economic viability of the entire division, and to support teaching and care to “impoverished patients” within the division. Similarly, an article in Healthcare Dive summarizes the comments of Misty Hathaway at Massachusetts General Hospital, a Harvard Medical School affiliate, describing the impetus behind its concierge program: “The primary motivation … she concedes, was finding ways to tap into new revenue sources. The entire margin from the concierge practice helps to fund programs like a substance misuse disorders clinic and community initiatives that might not otherwise have the same level of funding.”
The Tufts authors are commendably transparent in describing the origins of concierge medicine: “The growth of retainer medicine is emblematic of the disquieting trend away from traditional primary care,” they write. That trend has produced overworked, undercompensated primary care physicians, as well as dissatisfied patients. Thus, there are incentives for both “to move toward retainer-medicine practices.” Who can blame a physician for wanting to spend more time with each patient? And who can blame patients with complex conditions for paying extra to get the one-on-one attention they may need? Wouldn’t this be like blaming a ship’s passengers for running toward the lifeboats on a sinking ship?
Toward the end of Michigan Medicine’s panel discussion, Andrew Shuman, an otolaryngologist and co-director of the Program in Clinical Ethics in the Center for Bioethics and Social Sciences in Medicine, noted that at other institutions, luxury care programs “happen in the shadows.” Roughly a minute later, he added, “If we are truly using a Robin Hooding example, where we are taking philanthropic donations from those who have the capacity to do so, and reinvesting them in those who cannot, I think that is very clearly a transparent mission that we can get behind, or at least many of us can get behind.
“When this is opaque, though, I think is where we run into problems,” he said.
By spring, things still felt opaque to this University of Michigan English major, so I decided to look for data that would help me better understand how concierge medicine works at other health systems. I searched the academic literature, assuming I’d find case control studies comparing health outcomes for concierge vs. non-concierge patients, or comparing rates of health care utilization (number of prescriptions, tests, and referrals) among groups. Do concierge patients have shorter waits to see a specialist? How do non-concierge patients fare when their doctor decides to take part in a concierge program? And are revenues generated by concierge programs really helping to extend care to the wider community?
In the private, for-profit, sector, concierge programs often cite “proven” outcomes — though such assertions have been called into question. When it comes to studies comparing concierge to non-concierge patients specifically within the setting of an academic medical center, I found just one. It was published by researchers from Tufts, the University of Washington, and Blue Cross Blue Shield of Massachusetts in 2009, and it compared concierge and non-concierge patient satisfaction scores over a 12-month time period on a variety of indicators such as helpfulness of office staff, ability to get an appointment, and physician-patient interaction.
Much more abundant in the academic literature, it turns out, are voices pointing to a lack of data on the benefits of concierge medicine. In 2004, the surgeon James W. Jones wrote in the Journal of Vascular Surgery: “There is … no evidence that boutique medicine and surgery improve or do not improve outcomes.” In 2010, Michael Stillman wrote in Annals of Internal Medicine: “Yet until data demonstrate that the longer visits, ‘executive’ physicals, or annual ancillary testing offered by so many luxury practices yield better clinical outcomes, no one should … be allowed or led to believe that prompt or expensive care is necessarily the best.” And finally, in 2015, the American College of Physicians released a position paper noting that while retainer fees may cover special amenities such as extended patient visits and coordination with specialists, “No research is available to indicate the cost-benefit of such amenities.”
I started to wonder if there was a reason for that. Data on outcomes, after all, could open a Pandora’s box of ethical issues. If concierge patients fare better than their non-concierge counterparts, would health systems be obligated to offer this evidence-based medicine to all patients? And if concierge patients don’t fare better, would health systems be obligated to inform their patients?
As it stands, academic health centers market their concierge programs with a bevy of what seem to be deliberately opaque terms. Few actually promise “better” care. Instead, they use words like “enhanced” and “new model.” Concierge medicine programs also target “busy” patients — though presumably not those busy working two minimum wage jobs. I wrote to Michigan Medicine, asking if any faculty experts could speak with me about data supporting the efficacy of concierge programs. In particular, I wondered: Do they improve the health of patients who can afford to pay? And does everyone else benefit from trickle-down largesse? A spokesperson informed me that she was not arranging interviews on the topic. I also contacted Massachusetts General Hospital, Duke Health, and UNC Health Care with a series of questions, including whether they could point me toward outcomes data for concierge patients.
All initially promised to get back to me; only UNC did. Phil Bridges, a UNC spokesperson, wrote: “We are not prepared to speak to outcomes.”
Toby Citrin, a professor at the University of Michigan’s School of Public Health, appears to be chuckling at the question I’ve just posed in our video interview: Can the University of Michigan fulfill its mission without offering concierge medicine?
“Without Victors Care, our health system has grown enormously, is able to expand on a continuing basis, has built new health centers. Now, that doesn’t guarantee that that will continue in the future, but it seems to me that the system has proven that without stratification of this type, it can provide very high quality of care, can grow, make more money, expand, all those things. I haven’t seen a case made that absent Victors Care, this might slow down,” he said.
I reached out to Citrin after he published an op-ed titled “Victors Care does not belong at Michigan” in the Michigan Daily, the University of Michigan’s student newspaper. In that article, he argued that the stratification of care based on ability to pay is inconsistent with the goals of a public university. “What’s the next plan to capture revenue by further stratifying the University experience?” he wrote. Perhaps “concierge education?”
That might seem like an absurd slippery slope argument until you consider that in 2006, university faculty were busy protesting the incorporation of luxury boxes in the remodeling of Michigan Stadium, warning of “the growing stratification of our society and a sad corruption of our university’s defining traditions.”
In light of the blowback here at Michigan, the Victors Care website has redacted the word “concierge” from its homepage and replaced it with the term “direct primary care” — though that could well prove problematic in itself. While the terms are sometimes used interchangeably, they are not the same thing, with DPC arising in the 2000s as a way to address the problem of extending health care to the uninsured, not as a way to generate revenues by catering to elites. (Indeed, one DPC clinic owner here in Michigan told me that people are frustrated that the university is generating bad press for direct primary care by making it seem elitist.)
As for me, I’m still looking for data and for answers that offer more than chicanery. And in the meantime, I offer this sample of email correspondence with Mary Masson, a spokesperson for Michigan Medicine:
Me: Dr. Runge mentioned that specialists will eventually participate in [Victors Care]. By “specialists,” does he mean people outside of primary care? And if so, which in which specialties?
Masson: Victors Care specifically provides primary medical care. We do not have anything to announce about specialist care.
Me: Can someone please explain the connection between offering VC and bringing in philanthropy? Since the invites went out to people who have already donated to Michigan Medicine, one might assume they’d be happy to continue giving — even to vulnerable populations — without a special primary care program.
Masson: Victors Care is not a fund-raising effort. It is an optional way of providing primary care.
Me: Is Victors Care better than [the university’s] standard primary care?
Masson: [No response.]
Sara Talpos is a freelance writer whose recent work has been published in Mosaic and the Kenyon Review’s special issue on science writing. Sara has an MFA in creative writing (poetry) and is interested in the connections between science and literature. She taught writing classes at the University of Michigan for 10 years.
Comments are automatically closed one year after article publication. Archived comments are below.
My 36 year old single daughter is suddenly faced by a set of medical problems that are painful and potentially lethal. She waited one month to see her primary care physician and was seen instead by a nurse and a nurse trainee. They gave her referrals to three specialist practices (no specific names) and told her to make the appointments. Waiting times ranged from one to six months, with no one concerned at all that the logic of seeing a surgeon before one had a diagnosis from a GI or GYN doctor. She is a working woman with basic health insurance and on her own would not be able to afford the $6000 that her hospital charges for concierge care. I can afford to help her but found your article very helpful in sorting out the issues involved. The bottom line: we just need help–someone to answer questions, to set up specialist appointments in a logical way, to set up diet and other wellness regimess that will get her through the very anxiety-provoking wait times that seem to be unavoidable. Retired people like us spend $6000 on a winter cruise. I would rather spend that much on seeing my daughter through this very scary time, and despite my fury that the American health care system is so poor and so expensive, I am very grateful that big hospitals are providing this service, because it is a badly needed antidote to the current problems.
Exactly what DPC and Concierge medicine are designed for….to allow options. My only concern is the incorporation into big business and institutions…the very same reason for current healthcare failure. Find a physician seperate from big business…one who CAN and will speak the truth concerning your care. Big business, including the hospitals, are much to blame for the current healthcare crisis as they are motivated by money.
I have been a concierge physician since 2005. We have a three physician practice. Our fees are relatively low, age adjusted and range from $800 per year to $2,600. We have many pro bono patients based on economic need. I am the chair of the American College of Private Physicians, a porfessional society for concierge and DPC doctors. A few years ago I was asked to write a textbook section on concierge medicine for a book on medical professionalism, “Professionalism in Medicine, A Case Based Guide for Medical Students” published by Jefferson Medical College, and though a bit dated it is still useful. There are several published papers demonstrating the great benefits of concierge medicine, most done by MDVIP which draws its data from over 800 of its concierge practices. These studies for example show up to 90% reductions in hospital admissions and better outcomes for members than for matched patients with conventional care. I am surprised the author did not find these studies as they are common knowledge in my circles. I would be happy to talk to the author of this article any time.
Pay less for something and get less of it and/or a lower quality of it. Pay more for something and get more of it and/or a higher quality of it. We’re not outraged by this in any other aspect of our lives. Why should medicine be different? I don’t currently have concierge medicine, but I sure as heck want it to be an option.
Great article! I was super interested in the paragraph that begins, “These arguments reflect pressing health care concerns across the United States, which has a well-documented health care gap that falls along socioeconomic lines” and goes on to elaborate on some then vs now comparisons. Do you have sources for those stats? I promise, I’m not digging for dirt or anything, I just genuinely found those statements interesting/terrifying/disheartening, etc. and would like to see the original articles. Thanks!
Steven King: in no way was I equating concierge medicine with direct pay, as you will see if you reread my note. And, yes, DPC is definitely a way to go for those lacking insurance, but can afford the monthly retainer. I know that my physician has a number of patients who fit that demographic.
We must evaluate this appropriately as I believe there are assumptions being delivered in this article. First of all we have an obligation to give “appropriate care”. That is to give care where there is” time” to listen, diagnosis and treat…..but most importantly prevent the illness. We talk about equality of care and what most people want is equality with the top 10% not the bottom 10%. CDC recently published in 2016 that the US health care system is the 3rd leading cause of death. I do not want to give people more access to this type of system of rushed hurried care. When delivered appropriately we can lead our patients out of that sinkhole. When the third party payers dictate care such as government and insurance companies and dictate how much time you have to give to keep your clinics open in order to see the volume sufficient to the cover the high overhead. Most people do not realize that physicians cannot keep their doors open anymore in the current model. Most of that overhead is going to admnisistrative bodies to run the system. Most primary care clinics owned by larger healthcare companies are run in the red and lean on specialty and hospital care to balance the sheets. There are areas in medicine that I am proud to still say we provide exceptional care, however, in primary care we cannot provide effective and appropriate care in the models that employ most providers and physicians. I would be happy to share the biometrics in my clinic compared with the standard clinic data or national data.
Remember if you pursue and want standard of care medicine for the patients in your areas, then , you should expect standard of care results as we have seen the CDC data above. People make value choices all the time of lifestyle choices, from vacations, to the vehicles we own, to cable TV bills, smoking cigarettes, eating meal at resturants, elective surgeries, fashion appearel etc… I think to pursue a level of care that is backed by evidence and improve health status, DPC and concierge models eliminate the third party disrupters and bring the physician/patient relationship back to a level that can deliver health and sick care as we all imagine it to be.
Please don’t confuse Direct Primary Care with Conciere Medicine. True DPC practices are a great value for patients. DPC practices typically charge a nominal fee of $50-75/month with unlimited visits and greatly discounted labs and generic medications.
Equating a DPC practice with a Concierge one is the same as saying water and vodka are the same drink…they both are clear and will get you wet if spilled.
I wrote my doctoral dissertation on concierge medicine in 2008 and I included the various spinoffs available then. The ethical aspects of it were dicey and still are but, as we all know, there are the haves, the have nots, and the have mores. At that time there were only some 200 concierge practices in place, and I ultimately concluded it was too early to place any bets on it becoming a thing, that it might ultimately be just a passing mention in the history of medicine.
The irony of it all is that I find myself a patient in a direct payment practice which, while not nearly as deluxe as a concierge practice, better suits my medical needs. It also better suits my physician’s needs/desires, since she goes to Haiti annually for a week to care the Haitian people, as well as heading up a free clinic for the homeless in town. She and her partner have been available to my husband and me 24/7 and, unfortunately, we’ve had to make use of that availability on occasion. That I could get through to my physician immediately amazed the EMTs who were present. Lest I sound like one of the have mores (although I am, to some degree), the cost for the two of us is $1900 per year. That’s the cost of a latte a day which many spend without a thought. Priorities, priorities.
I do believe public universities who receive government funding should not be dabbling in concierge’s medicine. Now they have a hand in both pots. However, as a physician but also a healthcare consumer, I want this option for me and my family. We are not yet a socialist society where everyone is condemned to the same inadequate and lacking systems of education, healthcare and housing that the government can provide. If the affordable healthcare act taught us anything, it taught us that they will fill the gaps in healthcare with subpar care to cover everyone. Midlevel providers (oops, I’m supposed to call them Advanced Practitioners this week) replace primary care and now even the waits to see them are climbing. Government supplied healthcare is NOT the healthcare that the upper echelon wants. They are now calling us physicians “providers” so why not treat it as the consumer based product it really is? If I am providing and charging for a service, my services that require increased work, time or convenience should cost more. If the healthcare consumer (who used to be called a patient) wants more, why should that not be available? I for one would love to see private pay healthcare take off and essentially strip the power from the insurance companies.
Thanks for writing this and exploring some of the issues associated with concierge medicine. As a pediatrician in a primary care practice that takes basically all insurances equally (we are about half Medicaid or CHIP) the ideas of concierge medicine and to some degree direct primary care have never sat well with me. I too would love vto hear about outcomes data, hopefully there is some research somewhere that is starting to look into this.
Thank you for a timely, important article. There’s a further angle that I think warrants discussion regarding concierge medicine and academic settings. Currently 60% of undergraduate teaching at US colleges and universities is done by adjuncts, who get no benefits or health insurance. Thus the academic world is now engaged in actively exacerbating social inequity, particularly regarding medicine. Many adjuncts I know cannot afford health insurance. Under Obama-care the ones who earn below $48,000 annually do qualify for assistance, though it must be stressed that if you earn more than about $40,000 annually you don’t get much assistance at all. On the individual health care market, if you are over 50 health insurance now routinely costs $700-$1000/month, and that is with very high deductibles. Thus it is increasingly the case that adjuncts and other self-employed people (writers, journalists, Uber drivers, gig economy workers, people with modest middle-class incomes) may be paying easily a quarter of their total pre-tax income in health care costs. It is utterly immoral that public universities, or any universities, who claim to care about social justice, are promoting concierge medicine to a small group of elite faculty at the same time that they are hiring ever-more adjuncts without any health insurance.
great article. I am a Michigan alum, taught here for twelve years and started using the medical system in 1960. I am totally opposed to two tiered delivery of health care, which we already have, given the stats on who lives longest, but this would make it worse.
Wow, this is such a well-written article. You really care about our community and without being editorial present the evidence in such a convincing way. Concierge medicine does not belong here.
I’m a concierge doctor. I can tell you there are some seriously thorny ethical issues involved. They are not easy to resolve in either direction.
This is complicated by the fact that the insurance model has become unethical, as well as intolerable on it’s own.
However, I think that concierge doctors need to own the reality of the ethical implications (problems) of this form of practice. And socially we need to decide whether we are willing to abandon capitalism in regards to healthcare, or not… And that’s *not* an easy or obvious decision.
My only concern to this article is the idea of looking for evidence. Concierge medicine is new. We’re still adjusting, innovating. It’s a bit absurd to think that definitive evidence could be generated this quickly. It’s like looking at the “evidence” for open heart surgery in 1960… Every single attempt had failed, for many many years.
Between 1950 and 1955, 18 attempts at cardiopulmonary bypass were published. 17 of those patients died.
And yet, despite “evidence” to the contrary, DeWall persisted in trying again. Ultimately successful, he ushered in a new era of cardiac surgery that is only possible because he continued to tinker with a process until it worked as hoped… And *then* there was evidence.
Any other approach devolves into a combination of stasis and industry-funded pseudoscience (since individual physicians would be cut out of the innovation process).
This systematic re-tinkering is far too new to think that reliable evidence would be available, especially in the domain of primary care, since we are looking for lifetime outcomes, which, to paraphrase Atul Gawande in his piece, “The Bell Curve”, often hinges on seeing, on a daily basis, the difference between 99.5% success and 99.95% success.
I would add that all such innovation begins as cost-ineffective solutions.
I’m happy to discuss further if interested.
Totally sounds like the two-class health system from Germany – “normally insured patients” who have long waits and have to pay for some care out of pocket and “privately insured patients” who recieve appointments faster and have more extensive coverage
When my primary care physician at Washington University in St. Louis moved to a concierge service he also physically moved from the city of St. Louis to a wealthy suburb. I liked him a lot but I refused to follow him on ethical grounds.