








Does Science Support the ‘Wilderness’ in Wilderness Therapy?
Katherine Gibbons’ life turned upside down on the day in October 2018 when she skipped school, stole a liter of vodka, and drank much of it on the walk back from the grocery store. Her mother, who had been worried about Katherine’s erratic behavior for months, saw the 17-year-old was off campus through a phone-tracking app. She arrived at the school as her daughter stumbled in and was losing consciousness on the floor of the assistant principal’s office.

The school called 911. It was Katherine’s fifth emergency room visit over the preceding year. “It was clear that whatever we were doing here for her was not working,” said her father Mike, an executive at an infrastructure construction company with a thick crop of graying brown hair.
Her mother Erin is a stay-at-home mom who manages the family’s affairs out of their house on a four-acre property in the Chicago suburbs. “Either we were going to have to bury her — she was going to die,” Erin said, her voice breaking — “or we were going to have to do something dramatic.”
On the advice of a consultant specializing in teen therapy, they hired two strangers to come to the hospital and transport their daughter — semi-conscious — to Evoke Cascades, a wilderness therapy program more than 1,600 miles away in central Oregon. Katherine would spend the next 10 months in therapeutic treatment, including just over three months in wilderness treatment.
At Evoke, she lived out of a backpack with a small group of other teen girls and staff. Her days consisted of hiking, group and individual therapeutic exercises, cooking her own food, and sleeping outside under a tarp. It was cold and often rained or snowed — some days there was freezing rain. When she went to use the bathroom, she was required to continually call out her name so staff knew she hadn’t run away. At night, they collected everyone’s shoes for the same reason. Katherine had no access to technology and stayed in touch with her family through letters her therapist brought in and out during weekly visits.
“I was very mad,” Katherine recalled. “The first two days were really hard for me because I was freaking out. I was in denial.” She eventually transitioned to a therapeutic boarding school in Utah, where she stayed until just after her 18th birthday. She returned home last August.
Katherine is one of an estimated 5,000 to 6,000 adolescents who find themselves in wilderness therapy programs every year. These programs are distinct from traditional drug addiction treatment centers, and wilderness programs may require that incoming participants with a history of substance abuse be fully detoxed elsewhere before admittance. For the most part, it is the underlying emotional and behavioral problems — ones that parents have decided they are incapable of handling — that bring teenagers like Katherine to places like Evoke Cascades. Most start with wilderness therapy and move on to some other form of residential treatment, which can last a year or more.
Once plagued by scandals and charges of abuse and even deaths, the residential treatment industry has worked hard over the last two decades to reform itself, and stories of teenagers being handcuffed and assaulted or otherwise mistreated in fly-by-night “tough love” programs have largely — though not completely — disappeared from headlines. But even amid steady growth for the industry, some critics argue that such programs still suffer from one serious and fundamental shortcoming: a distinct lack of scientific evidence that they work.
Writ large, residential treatment takes a variety of forms, from transitional living facilities and boarding schools with regular therapy, to locked-down treatment centers with round-the-clock supervision. All are predicated on the notion that at some point, removing children from their home environment and introducing therapy in a new setting can improve outcomes for troubled youth. “Wilderness therapy” programs like Katherine’s add an additional component, pairing psychological counseling with a variety of outdoor activities, from simple hiking, backpacking, and camping, to more adventurous fare like rock climbing and skiing. They are frequently marketed as a way to get a child ready to be receptive to a residential program.
Many parents swear by these programs, insisting that they saved their children’s lives — and the Gibbonses are among them. “We haven’t seen her this good in three years,” Erin said of Katherine last February.
Proponents also say that wilderness and other residential treatment programs fill a niche that other treatment options don’t, providing long-term, intensive, often specialized care that helps young people reset and learn new coping skills. “We kind of fill the gap between some of the services that are out there,” said Megan Stokes, executive director of the National Association of Therapeutic Schools and Programs (NATSAP), the main trade group largely representing private-pay youth residential mental health treatment programs. “Some states have cut budgets for their public-pay treatment programs, [while] others don’t do residential.”

Critics of the industry, however, suggest that many well-meaning parents end up deciding on such programs for their children too quickly, while in crisis, and armed only with claims of efficacy provided by consultants and program operators who have a financial stake in the matter. Studies finding benefit from the forced removal of troubled teens from their homes for placement in residential settings are few, these critics argue. And while some research has suggested that residential treatment can lead to short-term progress for some children, there is little evidence that such an approach offers long-term advantages over therapy provided at or near home, and for a far lower price.
The science supporting the addition of a “wilderness” component to adolescent therapy is even thinner, critics say — and what exists is too often tied to trade associations and conducted by researchers with clear conflicts of interest. As it stands, wilderness therapy programs typically cost parents $500 to $600 per day for a period of weeks or months, plus several thousand for the enrollment fee. At the suggestion of staff therapists and other program operators, most adolescents also move on from wilderness therapy to other in-patient, residential treatment programs before transitioning back home. The Gibbons family estimates they spent more than $182,700 for Katherine’s 10 months of intensive treatment, counting fees to insurance claims specialists and attorneys. Of this amount, they’ve only been able to recover $32,200 in reimbursement. Still, they say it was worth it. “It was so hard,” Erin said of having her daughter away. “But we just want her to have a healthy future.”
Without firmer evidence that such expensive outlays are worthwhile, however, some experts argue that wilderness therapy programs remain at best an unproven experiment, and at worst, a pricey dose of snake oil. “It’s hard to make a case for spending a lot of money on a program for which there is no strong evidence,” said John Weisz, a professor of psychology at Harvard University who specializes in mental health interventions for children and adolescents. “From the state of the evidence that I’ve seen, we really don’t know whether wilderness therapy has beneficial effects or not,” he added.
The lack of scientific evidence is partly why the steep fees that parents pay for these programs are rarely covered by insurance. Families placing a teen in a more traditional residential mental health treatment center are the most likely to draw some amount of insurance coverage — though they are still denied regularly. Therapeutic boarding schools, which focus more on academics, are often only eligible for hourly therapy coverage.
But wilderness therapy is rarely covered — and some insurance policies specifically exclude it.
The industry is now actively working to change that by underwriting studies and even subsidizing academic journals in which to publish them. NATSAP and the Outdoor Behavioral Health Care Council, a trade group dedicated specifically to wilderness therapy, both fund research on the efficacy of wilderness therapy and similar programs — and they argue that they do so because no one else will.
“OBH Council programs believe it’s an ethical responsibility to do research to see how we’re doing and see how we can be better,” said Rick Heizer, owner and executive director of Evoke Therapy Programs (which runs Evoke Cascades) and chair of the trade association.
“I fully support doing more research,” he added, “and would welcome external research.”
Residential treatment programs that emphasize outdoor experience have a long history, and they would seem rooted in an idea that many people consider axiomatic: That venturing into the great outdoors, and working up an honest sweat amid the challenges of Mother Nature, can build character, restore self-esteem, and otherwise soothe a troubled mind.
Advocates often trace the lineage of these ideas as far back as the 19th and early 20th centuries, when, for example, tuberculosis patients quarantined in tents to separate them from the general population are said to have experienced ancillary benefits from simply being outside. In the early to mid-20th century, summer camps developed to provide therapeutic services for children. These ideas gained further traction with the advent of the progressive “experiential education” movement, spearheaded by the American philosopher and psychologist John Dewey, and later with the founding in Wales of the Outward Bound program in 1941. This marked the beginnings of so-called “adventure therapy,” which emphasized the restorative power of physical and mental challenges, stress, and getting out of one’s “comfort zone.” Wilderness therapy — nominally a sub-genre of adventure therapy — is described today as the integration of standard clinical and group therapy techniques with an outdoor or wilderness setting.
For much of the 1970s and ’80s, these burgeoning wilderness therapy programs operated without much government oversight, and some even drew government contracts by offering themselves as alternatives for juvenile offenders. Others focused on getting parents to directly enroll their children, which, over time, proved more lucrative, and by the 1990s the so-called “troubled teen” industry of wilderness and other residential treatment programs was widespread and profitable. Programs emerged throughout the country, and as far away as Mexico and Samoa. (With its easy access to nature, Utah became the industry’s geographical hub in the U.S., and today is home to more programs than any other state.)
It was during the 1980s and ’90s that the negative headlines relating to wilderness-oriented residential programs began to circulate, and they continued into the 2000s. Children died — from accidents and negligence. Some young people who came out of these programs alleged mistreatment and abuse. Parents subsequently sued, arguing they had been duped and swindled by program owners. Several programs lost their state licenses, or, caught in litigation about the death of a child, voluntarily shut down.
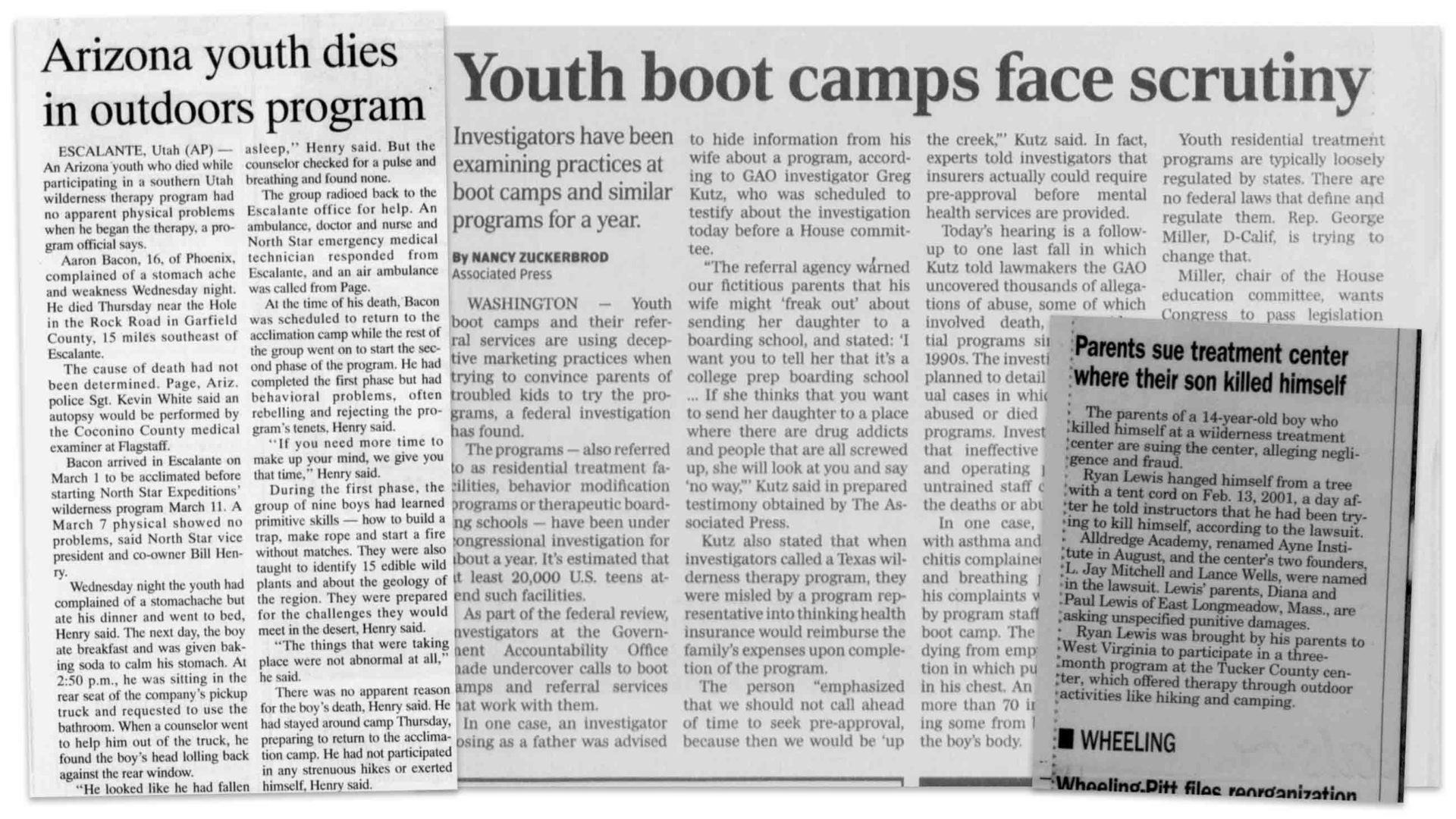
In one such case in 1994, at a bootcamp-style wilderness program called North Star Expeditions in Utah, staff decided that 16-year-old Aaron Bacon was “faking it” when he complained of severe stomach pain. He was punished with long, forced hikes, and deprived of food. Bacon died three weeks into the program after losing an astonishing 20 percent of his bodyweight. In 2001, 14-year-old Ryan Lewis reportedly told staff at Alldredge Academy in West Virginia that he was likely to harm himself, but his pleas were ignored. Left alone the next day, he hanged himself with a tent cord. And a year later, 15-year-old Erica Harvey died from heat stroke her first day at Catherine Freer Wilderness in Nevada, after staff failed to recognize her symptoms for hours.
With these and other allegations of abuse and negligence swirling, wilderness therapy eventually attracted the attention of Congress, which commissioned an investigation of the wider residential treatment industry by the Government Accountability Office. The parents of Bacon, Harvey, and Lewis all testified on Capitol Hill as part of a push for a bill to regulate the industry, bringing several representatives near tears. The bill passed the House with more than a two-thirds majority both in 2008 and 2009, but never made it to a vote in the Senate.
The economic downturn around that same time meant fewer parents had the resources to send their children to programs, and many operations closed. What was left of the industry began to remake its image into something more therapy-focused, arguing that most of the bad actors had been driven out of business. Meanwhile, state regulatory agencies have taken a variety of approaches to tighten scrutiny of wilderness therapy programs. California, for example, enacted legislation in 2018 that requires strict licensing of such programs, and specifically delineates participants’ rights. But even where licensure is required, problems can arise. Just this month, the Hawaii State Department of Health fined Pacific Quest, an outdoor therapy provider, for running two treatment facilities without having the proper licenses. And while there’s no official system to track bad actors and no national database of programs that market themselves as wilderness therapy, the industry’s leading trade group maintains a list of what it considers legitimate programs that are licensed or accredited — or working toward it.
Adolescents in such programs today have access to doctors as needed and regularly see a therapist — typically a psychologist or social worker. In many cases, they move through a level-based program that gradually grants them increasing privileges. And once a wilderness therapy program is completed, adolescents are often moved to other private therapy waypoints before eventually returning home.
This is the industry — the new, reformed industry — that Erin and Mike Gibbons encountered when concern for their daughter reached its apex.
The eldest of three, Katherine was an inquisitive and athletic child who loved playing with animals and riding her bike. She would line her toys up while the family watched Notre Dame football and push the cats, dressed in baby clothes, around in a stroller. But things got harder in high school. Anxiety that had started to develop in the preceding years got worse and Katherine’s grades dropped. As she spent more time using social media on her smartphone, she began to isolate herself.
Initially, Erin and Mike couldn’t tell if it was typical teen moodiness or something more serious. Then, in January 2018, Katherine skipped school and drove more than six hours to her aunt’s house in Ohio. She was pulled over on the approach to Columbus for driving over 100 miles per hour.
After she returned home, she and her family recall, a therapist diagnosed Katherine as bipolar. Over the next few months, Katherine was in and out of treatment programs, but in July, she attempted the drive to Ohio again. She switched therapists and medications multiple times. By October of 2018, Katherine’s medication had been changed again — to a stronger drug. “[The pills] made me super manic,” Katherine said. “They were supposed to be a mood stabilizer, and I was just not in the right mindset.”
She was drinking excessively, and the family called 911 several times. Between the calls, Erin met another mother at a yoga studio who had struggled with her own child. She recommended the Gibbonses speak to an “educational consultant” about finding treatment for Katherine. Such consultants, who are often former school counselors or administrators with mental health-related degrees, are typically the first contact that worried parents have with the industry. Most wilderness therapy program websites strongly recommend parents hire a consultant, though they stop short of requiring it. Nearly all of the families that spoke to Undark used one.
These advisors often become intimately involved not just in finding programs for troubled teens, but in coaching parents about wilderness therapy and related programs, planning transitions, and helping to handle other steps in the treatment process.
Erin says she called her consultant a day or so after being given her number. The woman listened to Erin’s story and told her she could help. They made plans for Katherine to be sent away for treatment at the end of that week — in the wee hours of Friday morning — but when Katherine was blacking out drunk at school on Thursday, Erin called the consultant back from the hospital. “It’s not going to work tomorrow,” Erin recalled saying. “She’s in the ER. It has to happen today.”
A few hours later, two transporters arrived — a man and a woman in plainclothes, one of them a former Marine. Katherine had been sedated, so they had the Gibbonses draft handwritten letters for when she woke up, explaining that they loved her and that the strangers were taking her to get help. Departures for treatment often move that quickly. Undark spoke to 18 families who sent their children to wilderness therapy and further residential treatment. For many, the turnaround between when they called a consultant — often referred by a friend or acquaintance in their network — and when they sent their child away was a matter of days or weeks.
“It was a leap of faith,” Erin said. “We just were like, ‘Either you guys take her and help her or she dies.’”

For Katherine, the transition was abrupt. “I had no memory of the hospital and I woke up in a hotel room and I didn’t know what I was — where I was. I was in a room with two random strangers,” she recalled. “I thought I was in human trafficking or something.” But the transport team was kind, Katherine said, and they gave her the letters, bought her food, and texted Mike and Erin regular updates during their journey to Oregon. But they never left Katherine alone and wouldn’t say where they were taking her beyond, “you’re going to get help.”
At the program, Katherine was given hiking clothes and outdoor gear, which all fit into a pack she would carry for the next several months. She was then driven to the high desert near Bend, Oregon. There, she joined a small group of teen girls with matching supplies and guides who rotated in and out on weeklong shifts.
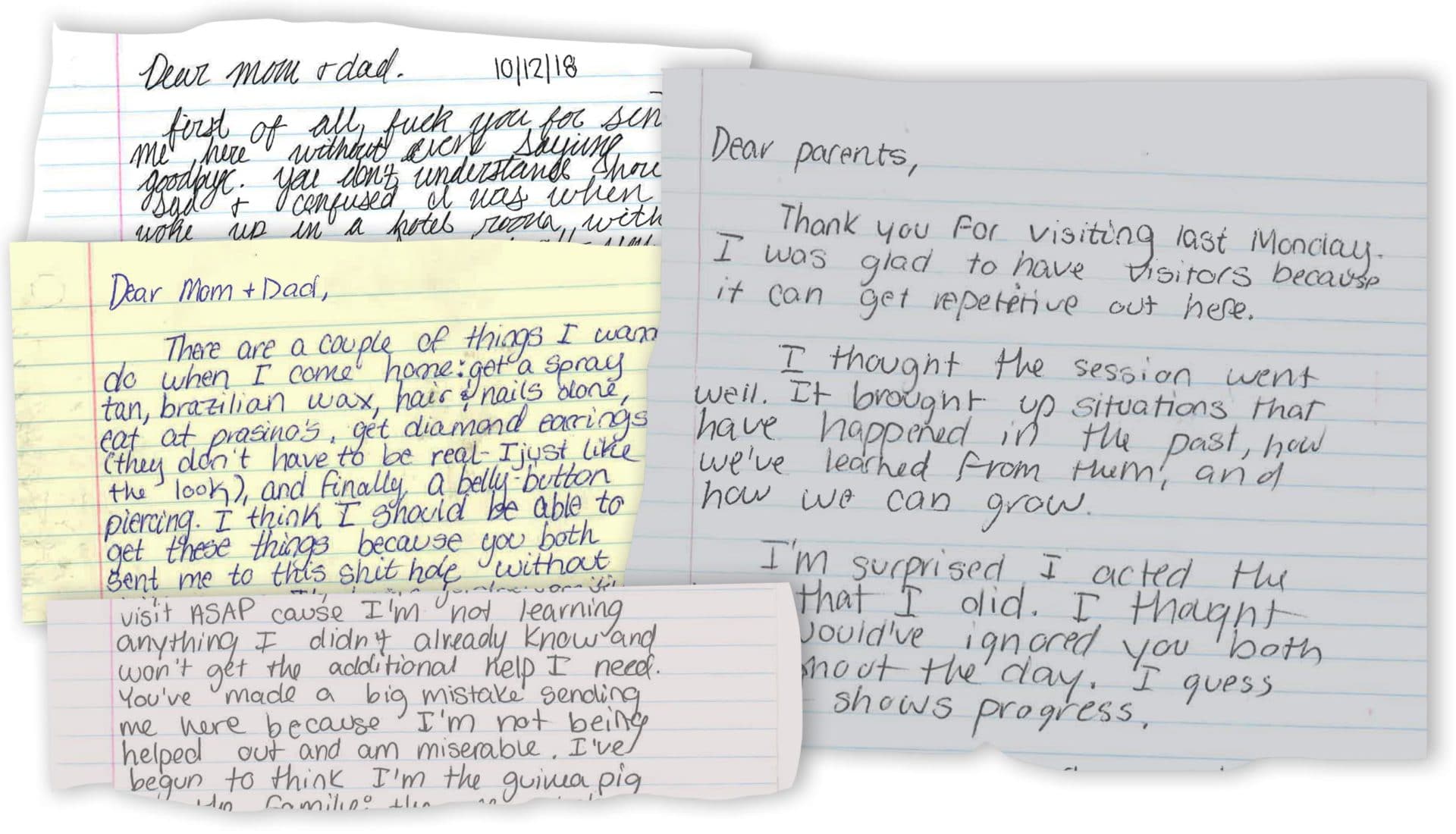
While athletic, Katherine was not an outdoors person, and her early letters home were full of curses, declarations of how she hated camping, and anger at being sent away without warning. “I was so mad,” Katherine said. “First I wouldn’t send my parents letters, and when I did it was like, ‘Fuck you. Fuck you. Fuck this. Fuck that.’ And there was one letter where I was like, ‘I’m moving to Ohio. I can’t live with you guys.”
Her letters got shorter and angrier when she learned she would not be going home after wilderness but to a therapeutic boarding school. Most adolescents who are sent to wilderness therapy go on to further treatment at therapeutic boarding schools or residential treatment centers — programs that provide therapy and academics in varying ratios, depending on the program structure and child’s needs.
“Students would be in my group when they’d get a letter from their parents that said they were going to go to boarding school and they’d find out that way,” said Amanda James, who worked as a wilderness therapy guide for a North Carolina program in 2016. It happened a lot, she said, recalling myriad awkward, sometimes painful, moments where she sat with a child as they processed the news that they weren’t going home anytime soon.
Indeed, roughly 80 percent of children and teens who attend wilderness therapy go on to a therapeutic boarding school or a residential treatment center, according to industry estimates. Some even go back to wilderness therapy if their program, parents, and consultant determine they aren’t ready for the next step yet. Meanwhile, the fees for all of this pile up: According to Mark Sklarow, CEO of the Independent Educational Consultants Association, a trade group for private-practice counselors, consultants typically charge between $3,000 and $8,000. While some may work only on a client’s initial placement, Sklarow says most continue to provide follow-up services. The Gibbons family paid theirs $7,250.
Consultants often recommend paid transport to the program — like the people the Gibbonses hired — which costs between $2,000 and $3,500 on average. When Katherine and her transporters missed their flight and had to get a hotel room for the night, her family covered the bill, spending more than $7,000 to get Katherine to her wilderness program. “Thank God we can make it work and we’re fortunate enough to do that,” said Mike, who built a spreadsheet tracking how much they spent on Katherine’s treatment. “If we weren’t, I don’t know what we would do.”
The Gibbonses planned early on to send Katherine to therapeutic boarding school after wilderness therapy, but not all parents are aware when they send their child away that the wilderness therapy program is just the start. “You think when you send your kid to wilderness, that that is the process,” said a mother in Massachusetts whose son went to wilderness therapy in May 2018. She asked not to be named to protect her son’s privacy. “But about six to seven weeks into it, you start hearing about ‘aftercare.’ Well, what’s aftercare? You quickly learn that wilderness is just triage.”
Her son came home from a residential treatment center in November of last year.
A second round of transportation adds expense, as do the therapeutic boarding schools and residential treatment centers where children end up, which can charge upwards of $8,000 (some nearing $20,000) per month. Visits — with the parents traveling to these programs, or the child coming home for brief stays — add up as well, and can involve a dozen cross-country flights over the course of a year.
It’s an additional financial burden and a much longer time commitment, but one that most parents come around to. “When I first heard this, I was pretty upset. Why am I bothering with wilderness? We got very skeptical,” said Donna McDonald, a California mother who sent her daughter to wilderness therapy in August of 2018. “Now I see it’s really smart.” McDonald said her daughter made great progress at wilderness, before moving on to a residential treatment center. She returned home last October.
McDonald, Erin Gibbons, and the Massachusetts mother are part of Facebook groups for parents whose children have gone to wilderness therapy and residential treatment. Members share experiences, support, and recommendations for consultants, insurance reimbursement services, and more. For the Gibbons, that online community has been vital. “We were second-guessing ourselves every second of the way,” said Erin. “But [Katherine’s] wilderness program has a great parent support system that really helped us keep above water.”
Staying afloat with a child inside this system can be difficult for anyone but the well-heeled. Insurance coverage is rare, though parents can sometimes get their local school district to help cover care of a special needs child. Getting that funding may require another consultant.
James, the former guide, recalled that most of the families she encountered were fairly wealthy. But, she said, between wilderness therapy and aftercare, it’s easy for families to end up spending more than they planned. “I think parents can see that once they’ve gone down a treatment route, it won’t be worth the investment unless they go all the way,” she said. “That’s when it really becomes unfair to families.”
Families are known to have tapped college funds, taken out second mortgages, or dipped into inheritances to cover costs. For those who can’t make the finance work, program websites advertise health care loan companies and insurance appeals services.
One such service based in Utah, Denials Management, has been leading the charge to increase insurance coverage for wilderness therapy. Run out of a suburban office park near Salt Lake City, with a view of the Wasatch mountains, the 30-person appeals company has filed thousands of wilderness therapy insurance appeals since 2015. According to data provided by Mary Covington, the company’s president and leader of the campaign for coverage, between 2016 and August of 2019, Denials Management earned $4.65 million for families in wilderness therapy coverage, with that number increasing every year.
She has partnered with the industry and industry-tied researchers on the campaign and has been working with lawyers since 2017 to bring lawsuits, many of them class action, for insurance coverage of wilderness therapy around the country. They argue that insurance companies must cover wilderness therapy under the federal Mental Health Parity and Addiction Equity Act, as amended by the Affordable Care Act, to provide coverage for mental health care comparable to the medical coverage of a plan.
“The goal,” said Covington, “is to get wilderness entirely accepted by the insurance industry.”
Of course, one of the reasons insurance companies deny coverage is because they still consider wilderness therapy to be an “experimental treatment” without scientific evidence that it works.
In a 2016 letter, Oxford Health Insurance, part of United Health Care, defended its denial of coverage for a Utah-based wilderness therapy program, stating that “wilderness therapy programs are not considered evidence-based treatment.” A lawsuit against the insurer was dismissed in 2018. Blue Cross Blue Shield of Massachusetts, Aetna, and Cigna have also been sued for a lack of coverage of wilderness therapy, though the companies have countered in those cases that such treatment was specifically excluded in the plans the plaintiffs were covered by. Still, some cases have been decided against insurers or have resulted in settlements.
“If a licensed psychologist is coming in and giving weekly therapy sessions, and then they also have the daily activities, and then patients improve, well how do you know it’s not just due to the licensed therapy sessions?” asked Paul Crits-Christoph, a professor of psychiatry at the University of Pennsylvania’s medical school who studies outcomes for various mental health treatment approaches. “Why should we be reimbursing?”
While there are several trade and nonprofit organizations related to various aspects and forms of outdoor therapy, the real nerve center for research relating to wilderness therapy today is the Outdoor Behavioral Health Care Center, established at the University of New Hampshire in 2015. It was a rebranding of the Outdoor Behavioral Health Care Research Cooperative, formed in 1999, which had grown out of a concerted and decades-long effort by several stakeholders — principally program owners — to restore the reputation of wilderness therapy following the scandals of the 1980s and ’90s.
The OBH Center is headed up by Michael Gass, a professor in the Outdoor Education Program in the Department of Kinesiology at the University of New Hampshire. Gass conducted research for the National Association of Therapeutic Schools and Programs for years and serves as director of the its research database. The OBH Center’s stated mission is “to advance the outdoor behavioral health care field through the development of best practices, effective treatments, and evidence-based research.”
The center currently has seven researchers, all of whom have worked in or have strong ties to the industry. Wilderness therapy’s primary trade group, the Outdoor Behavioral Health Care Council, issues accreditation to members — including Katherine’s program, Evoke Cascades — using metrics developed in part by Gass. The OBH Council has provided the research center with at least $1 million in funding since 1999, according to incomplete data gathered from researcher CVs, financial disclosures, and public records act requests.
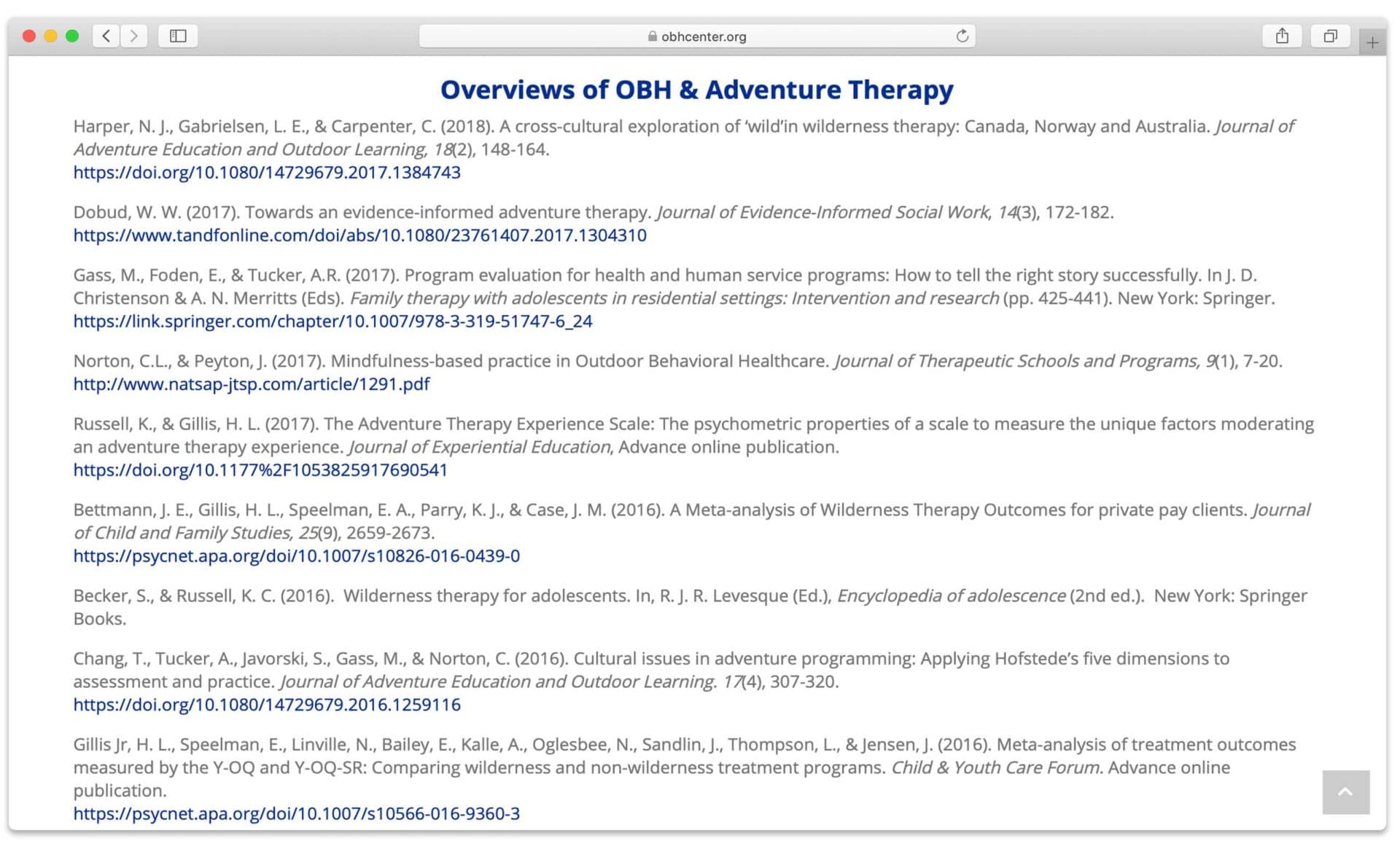
The OBH Center lists more than 120 publications on its website, many of them related to the broader field of adventure therapy. While Undark has not independently verified which of these studies independent scientists would consider “outcome studies,” which empirically evaluate the results of a given therapy approach — in this case, wilderness therapy or similar programs — fewer than half appear to fit this criteria. The rest include book chapters, narrative case studies, academic discussions of research challenges, or examinations of outdoor activities or therapy as used by populations beyond so-called troubled teens — such as veterans, children of adults with cancer, and even elementary school students. A review of studies from ProQuest, PsycInfo, and Scopus — databases recommended for psychology research — turned up just 24 additional papers that appear to look at outcomes of wilderness therapy in some measure.
Experts consulted by Undark raised several questions about the quality of this body of research. Several noted a lack of follow-up studies to show how effective wilderness therapy is over time. Many others pointed to the absence of control groups — study participants who do not receive wilderness therapy — in most of the published research. Without a control group, said Weisz, the Harvard psychologist, it is difficult to know if any treatment is effective. People often seek treatment when problems have gotten to their highest level, he said. “So by regression to the mean over time, they’re likely to be better six months later just because they started at their peak.” That’s why it’s important to have a control group, Weisz said. “Some of how much better they are is the natural time course of the problem.”
A control group study on wilderness therapy that the OBH Center calls “groundbreaking” was published in 2018. The study’s lead author, Steven DeMille, is the executive director of a Utah wilderness program, Redcliff Ascent. Gass and Anita Tucker, the OBH Center’s associate director, were co-authors. The study compared parent-reported outcomes for 60 recipients of wilderness therapy at Redcliff Ascent with outcomes for 60 patients who received what was considered “treatment as usual” — described as one to five hours of individual and family therapy. The analysis concluded that wilderness therapy provided better outcomes.
Asked by Undark to review the study, Alan Kazdin, a research professor of psychology and child psychiatry at Yale University, disagreed with this conclusion. “I don’t think they have the evidence,” he said, noting that wilderness programs combine therapeutic practices that are, in fact, similar to those at work in more traditional, “treatment as usual” therapies, albeit in a wilderness setting. Given this, the real question, Kazdin suggested, is not how one to five hours of therapy compares to an immersive, round-the-clock residential program, but whether the wilderness part of these programs matters.
As designed, Kazdin suggested, the DeMille study failed to answer that question. “The appropriate control group is not treatment as usual, which is fine in many studies,” Kazdin said, “but really is separating out the wilderness from the other components. Many of those other components would have been fine all by themselves.”
Other experts found DeMille’s dual role as study leader and executive director of the program being studied a matter of concern. Both DeMille and Brett Talbot, another co-author and then the senior director of quality and research at DeMille’s wilderness program in Utah, did clearly declare their affiliations in the study itself, noting that they were not a part of the data analysis — though they did participate in other ways. This was still problematic, said the University of Pennsylvania’s Crits-Christoph. “It looks like they’re overselling it,” Crits-Christoph said, “and that’s worrisome given the huge financial side of this — particularly that DeMille is one of the people on the inside making money off of it.”
Nonetheless, DeMille’s control-group findings were used in another study last year examining the cost-effectiveness of wilderness therapy in adolescents with substance use and mental health issues. It was led by Gass alongside Tucker and Talbot. (In the study, Gass declared a conflict of interest, noting a small part of his salary is paid for by the OBH Council and NATSAP. “All other authors of the manuscript declare no conflict of interest,” the paper stated.)
The study analyzed DeMille’s findings alongside cost and completion rates for both wilderness programs and “treatment as usual.” Gass defined treatment as usual more broadly than DeMille — including everything from outpatient care to detoxification programs, residential treatment, and hospital stays. Then he calculated the cost of treatment as usual based on the average cost of 10 randomly selected, non-wilderness NATSAP member programs. The vast majority of NATSAP programs are residential treatment centers or therapeutic boarding schools, which are generally as, if not more, expensive than wilderness therapy. They are also typically longer, and children are more likely to leave early. Gass did not break down cost or completion rates by program type within the treatment as usual group.
“They are doing a sleight of hand with those studies,” said Crits-Christoph. “It may well be that wilderness therapy is less expensive than residential treatment. But residential treatment would not likely be the alternative for many of the individuals who go to wilderness therapy.”
Every expert consulted by Undark noted that wilderness therapy has yet to be subjected to a randomized controlled trial — the gold standard in scientific research. Without randomized trials, where participants are assigned randomly to control and treatment groups in a study, and replicable results, it is difficult to determine how effective any treatment is. Randomization also helps protect against potential bias in studies, such as researchers with allegiances to certain therapies or facilities, said Raquel Halfond, an expert on child and adolescent research with the American Psychological Association. “Bias can essentially make someone think that an outcome is due to something that it’s not actually due to,” she cautioned.
Gass said that he and his colleagues — including those associated with the trade group — have not attempted randomized trials for ethical reasons. “There’s been a decision made by the Council that we were not going to utilize randomization because that would mean withholding treatment from kids that needed it,” he said. “And we understood that that lack of randomization would be criticized by some colleagues, but we felt that ethically we did not want to go and utilize that form of research design.”
Other researchers found that explanation difficult to fathom. Ethical issues are always a concern with randomized controlled trials, said Kazdin, but researchers have successfully conducted them not just for mental health, but on many important scientific topics, even “cancer, HIV, and other situations where there are — have been — huge ethical issues.”
Whatever the merits of the outside critiques, there is little question that owners of wilderness therapy programs see the OBH Center’s publications as a boon, and they are frequently touted in facility marketing materials and on their websites, where they are used to underscore the “evidence-based” bona fides of the program. Several parents told Undark that seeing this research helped to cement their decision to send their child into wilderness therapy.
Heizer, the owner of Evoke Therapy Programs, said that posting research online isn’t meant to be deceitful. “I would call it ‘this is our research’ and I feel like that’s what we’ve done,” he said. “I don’t feel I’ve said ‘This is independent, 100 percent unbiased research.’” Rather, he added later, the research is done to advance the field and improve accessibility, not to manipulate parents. “I would also challenge that there are few parents who would send their kids to one of our programs who [say] the research had anything to do with it.”
But Robert Friedman, a professor emeritus in child and family studies at the University of South Florida and one of the founding members of Astart, or the Alliance for the Safe, Therapeutic, and Appropriate Use of Residential Treatment, a group of psychologists, psychiatrists, lawyers, parents, and others who helped bring industry abuses to the attention of Congress in the 2000s, disagrees. “If you go onto program websites, you’ll see how the research and evaluations that are done by the programs are used,” he said. “They’re really used to promote the programs and generate more business for the programs, much more so than they are to really get an independent sense of how well are they working.” On its website, NATSAP encourages programs to join its research project, noting that such programs will be able “to include the term ‘research-designated program’ and add the research designation logo (to be designed) in their marketing.”
Several critics pointed to other therapy approaches that are supported by more rigorous research. One, called multisystemic therapy, involves a three to five-month program for at-risk children and adolescents, with 24/7 on-call therapists who work with youth in their home, school, and community. Through more than 70 outcome, benchmark, and implementation studies, most of them conducted by independent researchers and 26 of them randomized controlled trials, multisystemic therapy has been found effective at treating problem sexual behavior, child abuse and neglect, substance abuse, and emotional disturbances — issues many wilderness therapy programs also say they treat. Thousands of families have participated, the research has been replicated, and follow-up studies have lasted as long as 22 years.
Another highly regarded, evidence-based therapy approach, called interpersonal psychotherapy, aims to treat adolescent depression in a three- to four-month program. Studies on its efficacy have been published in the Journal of Consulting and Clinical Psychology and the Journal of Clinical Child and Adolescent Psychology — two peer-reviewed journals run by the American Psychological Association.
This is in contrast to the research promoted by the OBH Center, much of which has been supported in part by the OBH Council, and published in one of two journals — the Journal of Therapeutic Schools and Programs and the Journal of Experiential Education — that are also peer-reviewed but were founded by related trade groups that provide financial support.
These and other aspects of the wilderness therapy research ecosystem have long made many critics skeptical of one central aspect of the approach: It requires exporting a child to a setting far from home, versus keeping them at home or in their own communities, as with multisystemic therapy, interpersonal psychotherapy, and other evidence-based therapies. That doesn’t mean wilderness therapy isn’t effective, of course.
“We have no idea if wilderness makes a difference. I’m not saying wilderness doesn’t — that’s different,” said Kazdin. “I’m not [saying] that. I can only say it hasn’t been shown to make a difference in these studies.”
Weisz was less circumspect: “This is sort of a separate world from the world where people actually do randomized trials and test rigorously to see what works,” he said. “There are multiple reasons why these programs — wilderness and similar programs — are not being tested in that way. One is that there’s no financial incentive to do it.”
Responding to questions from Undark based on these and other criticisms, Gass was firm but diplomatic. “I’ve consciously made an effort to utilize the center to make it independent from organizations.” He added that while he is still on the board of NATSAP’s journal and provides advice when asked, he no longer publishes there and has not reviewed a manuscript for it in three years.
Gass also said questions from Undark about the OBH Center’s ties prompted him to add an ethics statement to the center’s homepage. It describes all OBH Center research as being vetted by the University of New Hampshire’s Institutional Review Board, declares its independence and commitment to funding disclosures, and delineates the Center’s major underwriters, including UNH, federal and state funding, as well as the OBH Council and NATSAP.
Gass called it “probably one of the strongest statements I’ve seen on any research enterprise — a code of ethics of that level.”
At an August 2019 conference organized by the OBH Council, Gass gave a presentation about insurance accessibility with Covington — the president of Denials Management — and Brian King, a Democratic state representative from Utah and one of the lawyers bringing lawsuits for insurance coverage. Their slides outlined eight goals on the quest for coverage, including “pursue litigation,” “media exposure/get the word out about OBH,” and “get scientific articles concerning OBH published.”
When challenging a denial, Covington will often send a packet of dozens of wilderness therapy studies along with the appeal, or submit them in court if the case becomes a lawsuit, she told Undark. Gass will tailor the list of studies for her based on what the insurance company is arguing in each case.

If a company says wilderness therapy is “experimental,” Gass writes a letter arguing the insurer is using bad information to evaluate the program, he and Covington explained. In one February 2019 letter, which Covington sent to insurance giant Cigna, he wrote, “There is more recent and rigorous research evidence that finds OBH is safer, more effective, and less expensive than treatment as usual for these clients.”
Whatever the veracity of that statement, there is little question that the wilderness therapy industry is growing. Today, programs often have a parent company that owns at least one other wilderness program, and often other residential treatment programs. In the last two years, at least three new wilderness programs have opened and several others have expanded their offerings. And while the federal bill aimed at bringing oversight to the industry has continued to be put forward for years, its original sponsor has retired and it has not gotten a vote or hearing since 2009.
Meanwhile, the youth mental health crisis in the country has grown, with more young adults and adolescents experiencing serious psychological distress over the past decade, according to a nationally representative government survey.
James, the former wilderness therapy guide, believes such programs may well be the best options for teenagers who need to get out of their environment, especially if their lives are potentially at risk. But she saw the teens for such a short period of time it was impossible to know what effect it had on them. “I wish that I knew that it helped because the students do go through a lot when they’re there,” she said.

For their part, the Gibbonses feel they made the right choice; Katherine, both parents and daughter argue, needed the time and space for intensive therapy. At the wilderness program, her family says a psychological evaluation showed she had been misdiagnosed as bipolar; she actually had anxiety. She got off her previous medication and focused on learning to manage her anxiety. The family agrees she has improved a lot.
For Mike and Erin, it’s like they got their daughter back. “We’re so proud of her. She’s done such an amazing job, really working hard,” Erin said, beaming at her daughter across the couch.
Katherine came home in mid-August, just in time for her final year of high school. The therapeutic boarding school wanted her to stay through the first week of October, but Katherine was determined to attend her whole senior year. Her parents agreed to bring her back early — they wanted her home, too.
Reflecting on the past year, Katherine has mixed feelings. “I think treatment did help me, ’cause I don’t know where I would be if I hadn’t received it. But during the time I didn’t like it. Of course I didn’t, no one does, unless you have a very bad family life, but I just wanted to go home every single day.”
When she did, she said she was nervous after being away for so long, but back in her house with her family and her pets, most of the anxiety has disappeared. Her parents let her choose where she wanted to finish high school, and she spent the last week before classes working on her college applications. She’d already started her admissions essay at therapeutic boarding school.
Her top choice is the family alma mater: Notre Dame. It’s where her parents met.
“I really resented my parents for sending me away,” she said over the phone weeks later as she prepared to go to yoga with her mom. “I thought they just didn’t want to deal with me, but it turned out they didn’t know how, because I was in such a bad place, and all they wanted to do was help me.”
Adiel Kaplan, a New York City-based reporter, began reporting this story as a fellow with the Toni Stabile Center for Investigative Journalism at Columbia University. She has previously covered the environment and local government for InvestigateWest and the Miami Herald.
Comments are automatically closed one year after article publication. Archived comments are below.
Deberiais publicar muchos mas articulos como este. Muchas gracias, Un saludo
Sound research matters. I am a clinician who has practiced an evidence-based, intensive, in-home therapy model with teens and families for over a decade. So many parents struggle without the high level of support they need to parent kids who are hanging with troublesome peers and acting out. There is no easy fix. Changing deeply entrenched patterns takes collaboration, planning and deep commitment, but it pays off in the long run. Many of the parents I work with think boot camp/out-of-home placement will “fix” their kids and they’ll return home one day forever changed. We aim to help the family make the changes they desire in their own home, in their communities. Raising kids is tough, and I feel for parents whose experience is way more challenging than they expected. For some kids a wilderness camp may “work”, but without solid, independent studies it’s hard to know.
I guess the author doesn’t have Children. Certainly not those struggling. Maybe she considers funerals a cheaper and better option.
Wilderness “therapy” ruined my life. Five years later I’m still dealing with the trauma from it, and so is everyone else I know that ended up at various wilderness torture camps. 90% of these places are dangerously abusive and designed to break kids down for zombie-like compliance. It is not therapy, and it literally kills children.
I think the title of this article is somewhat unfortunate and misleading. The title of this article suggests that the authors are evaluating the impact of wilderness on wilderness therapy programs and I was excited to see what they found. Unfortunately, this article isn’t really about the impact of wilderness. This would be difficult to measure as there are so many variables conflated in these therapeutic programs, including: experiencing nature; primitive living skills and the collaborative social environment; forcing people to participate – in a potentially trauma inducing fashion; isolation from social media / electronic devices; an audience with significant behavioral and mental challenges; and many more.
As a former outdoor instructor who led wilderness programs for schools like the National Outdoor Leadership School (NOLS) I know that immersion in WILDERNESS and SOCIAL WILDERNESS EXPERIENCES have a very positive impact on most people who participate. These are non-therapy programs that are populated by people who choose to participate. For my part, I will never doubt the powerful potential of well run and ethical wilderness therapy programs. And, they alone, will never be enough to support people in such deep and complex need.
Great article, balanced and fair. We chose wilderness therapy for our child, and it was life-saving, life-changing. Totally support this approach when nothing else works.
Bravo!!!! Great piece!!!