








For the Uniformed Public Health Service, Existential Questions
In Atlanta, people don’t often recognize Commander Adam Lofton’s uniform. Now and again, someone at a gas station will thank him for his service, but he’s pretty sure they think he’s either headed to a nearby Air Reserve base or returning from the Army installation at Fort Benning, about two hours away. Years ago, while wearing a previous version of the uniform, he remembers being mistaken for a pilot: “Where you flying to today?” someone asked.
But in places that have been flattened, flooded, sickened, and oftentimes ignored, everybody seems to know what his uniform means. When he was deployed to New Orleans after Hurricane Katrina, he was out for lunch with some colleagues when another diner picked up their check. The buyer came to their table and thanked them for their service. “I felt the need to say, ‘We’re Public Health Service officers,’” says Lofton, “assuming they probably thought we were military.”
“Oh, we know exactly who you are,” Lofton recalls the patron replying.

Among other duties, the U.S. Public Health Service places medical providers in underserved communities throughout the United States.
Visual: U.S. Public Health Service
During a 2017 deployment to Puerto Rico after Hurricane Maria, he never once had to explain his dark blue uniform with his name stitched in yellow-gold over the right chest pocket. Even in the rural areas, people knew what it signified: Lofton is a member of the Commissioned Corps of the U.S. Public Health Service (PHS). It is one of the United States’ seven uniformed services, and one of the two that does not bear arms. Many Americans have never heard of the Public Health Service — today a division of the Department of Health and Human Services (HHS) — but a light bulb sometimes comes on when they hear the Corps is overseen by the Surgeon General.
New Corps members don’t join fresh out of high school or slog through boot camp, and there are no Public Health Service bases, camps, forts, or combat centers. Rather, professionals are considered for the Corps on the basis of specialized training in a field with public health applications. Nurses, pharmacists, and doctors comprise more than half of the service, though dentists, engineers, and even veterinarians are among its ranks.
They are scattered across 22 federal government agencies, with the highest numbers in the Indian Health Service, the Food and Drug Administration, and the Centers for Disease Control and Prevention. They provide much needed care on America’s impoverished Indian reservations, and they deploy to disasters, disease outbreaks, and all manner of other public health emergencies. The Corps deployed more than 1,460 officers in the aftermaths of Hurricanes Harvey, Irma, and Maria, and staffed a field hospital for infected health care workers during Liberia’s 2014 Ebola outbreak. More recently, officers led an effort to reunite migrant families separated by the Department of Homeland Security at the U.S.-Mexico border.
In short, they seek to fulfill the Corps’ stated mission to “protect, promote, and advance the health and safety of our nation.”
That’s a noble calling, but its very gravitas belies a less sanguine reality: Despite its 130-year history, the Corps in latter decades has operated under a pall of derision and threats to its very existence — some of it unfair, defenders say, but much of it earned, according to critics, whose voices are gaining new urgency under the budget-cutting administration of President Donald J. Trump. Detractors argue that there is scant evidence that the Corps fulfills its primary mission well enough to justify the cost of keeping its members in uniform. Mobilizations of service personnel are sluggish, disorganized, costly, and, worst of all, critics say, redundant: Other better-funded organizations already do what the Corps does, they say, and arguably more quickly and effectively.
I am familiar with these sorts of criticisms because I am a practicing physician and former CDC-based Commissioned Corps officer myself, and I was both privy to the internal strife and witness to the Corps’ frequent mismanagement. I am also aware of these problems because numerous former colleagues at the PHS, as well as people in ancillary agencies that have worked with the Corps over the years, have told me so — though most refused to go on the record for this story for fear of compromising their current positions or otherwise risking long-distinguished careers.
But the challenges facing this little-known federal service are well-documented in the public record. Calls for its dismantling reach back decades, and while Corps personnel have been instrumental in nudging forward key public health initiatives leading to, for example, the Safe Water Drinking Act and Clean Air Acts, the PHS has also found itself embroiled in controversies, including the infamous Tuskegee syphilis study of 1932. Meanwhile, the Corps has long been beset by underfunding and organizational reshufflings, much of it on the basis of a perception that it doesn’t quite belong in the company of its sister services under the Department of Defense and the Department of Homeland Security.
That perception arises in part from a decidedly unmilitary-like command structure, wherein the uniforms and the military adjacency of the Corps are seen in some respects as mere theater — particularly given that few if any officers are ever forced to deploy if they don’t want to. Indeed, the notion that the Corps is “military lite” has followed it since the latter years of World War II, although whether that perception is the cause or effect of its problems is a murky business. Funding for Corps operations is extremely sparse compared with that of the armed forces, and every decade or so, a government report questions the organization’s use of resources, often resulting in cuts to its budget and reorganizations of its already-inscrutable command structure.
A 2016 promotional video details the history and origins of the Commissioned Corps of the U.S. Public Health Service.
After the 2016 presidential election, internal Corps communications indicate, the federal Office of Management and Budget (OMB) planned recommendations to eliminate the Corps altogether. That recommendation was eventually downgraded, resulting in a proposal to slash the Corps’ size by nearly 40 percent. The proposal’s authors wrote that the organization should “civilianize officers who do not provide critical public health services or support in public health emergencies” — widely thought to indicate that officers like Lofton, whose day jobs are non-clinical, will be the first to be cut.
Lofton was an Army Medical Service Corps officer before he joined the Public Health Service. In the Army, he told me, one thing was clear: “In order for a medical mission to be successful, there are a tremendous amount of ancillary resources that are necessary to enable that mission. And the very same is true with the Public Health Service,” he said. Without logistics, operations, and planning, the delivery of medical care will not succeed. “It’s just paramount,” he said.
Previous threats to the Corps have decreased its funding, but the current proposal is seen as more menacing, largely because it comes from an administration that has proved its willingness to defund even popular and effective programs in the name of fiscal conservatism. While vague, the most recent budget request for HHS indeed signals an effort on the part of the Corps to adhere to the OMB’s vision of “modernization,” with a leaner, more clinically-focused organization. But if cuts are enacted, proponents of the Corps say they would render it unable to meet the day-to-day health needs of thousands of people who, knowingly or not, rely on Public Health Service personnel. And the timing, these advocates say, couldn’t be worse: As a warming climate leads to more frequent and severe natural disasters, and as rising trade and travel contribute to more frequent infectious disease outbreaks, the need for emergency responders is only expected to go up, not down.
At the same time, dueling missions and internal cultural and structural weaknesses have historically prevented the Corps from functioning well when it tries to behave like a health emergency response agency, critics say. As such, the Corps now finds itself tasked with proving to detractors that, given the right resources and personnel, it could be the organization it has long claimed to be — even if nobody notices.
The Commissioned Corps was initially conceived in 1870 as a medical cadre to serve inadequately staffed marine hospitals moldering along American waterways. Surgeon General John Maynard Woodworth led the service, dressing his doctors in uniforms and deploying them to bedsides the way soldiers deployed to battle fronts.
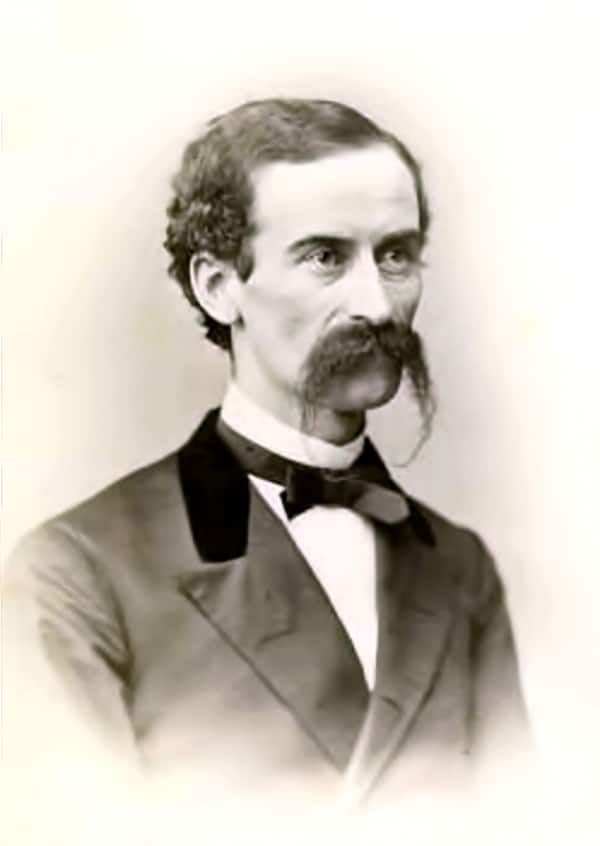
Surgeon General John Maynard Woodworth led the first iteration of the Commissioned Corps when it was first conceived in 1870. It would take many administrative and organizational forms in subsequent decades.
Visual: Wisconsin Historical Society
The force’s late-19th century formalization coincided with major bacteriology discoveries in Berlin and Paris, and its public health-minded officers took on a patchwork of duties broadly targeting the scourges of infectious diseases: among other duties, they oversaw vaccine production, fought outbreaks, and improved outhouses. They also became doctors to Americans on the fringes, including residents of the Louisiana Leper Home and federal prison inmates. Native Americans were added to the roster in 1928, the same year the Meriam report, a survey of conditions on reservations in more than two dozen states, excoriated “practically every activity” of the U.S. government related to Indian health. Many programs initiated by the Public Health Service later developed into agencies including the Centers for Disease Control and Prevention and the National Institutes of Health.
In the early 1940s, after a massive expansion in the budget of the PHS and the size of the Corps, Surgeon General Thomas Parran introduced legislation to modernize its bureaucracy and clarify its institutional identity. Parran’s move was met with resistance by hawkish legislators who disputed whether Corps officers were entitled to be treated as other uniformed servicemembers despite not routinely deploying to battle. As one Congressman observed, Corps officers were “neither fish nor fowl,” covered neither by civilian nor armed forces benefits — but the War Department, the Veteran’s Administration, and the precursor to OMB resisted giving Corps officers military benefits because in their view, Corps members were civilians.
In the spring of 1943, the chair of a Senate subcommittee argued the lack of benefits jeopardized the Corps’ ability to recruit and retain personnel to perform vital public health functions. Later that year, President Franklin D. Roosevelt signed the Public Health Service Act of 1943 into law, authorizing limited or full military benefits for Corps officers dependent upon their wartime service.
During World War II, the Corps was even temporarily declared a military service, though that still didn’t mean legislators took the organization — or its leadership — seriously. Although officers and their agencies had always been managed by a Surgeon General who had come up through the Corps’ ranks, a 1968 overhaul of the Corps’ organizational structure reassigned his duties to the Assistant Secretary for Health, known as the “ASH” — a political appointee and advisor to the secretary of what would eventually become the Department of Health and Human Services, HHS.
It was a mortal wound to the authority of the Surgeon General, says John Parascandola, the Public Health Service historian from 1992 to 2004. “That’s when people begin questioning, you know, ‘Why do we need this uniformed service? Why can’t they just be civilians?’”
To casual observers, the change to the Corps’ structure probably looked like just another spasm of administrative reshuffling. In actuality, it decapitated the organization and eviscerated its chain of command. Corps officers now reported to a politically motivated leader who most often was not a veteran of its organization nor beholden to its mission, and the Surgeon General was relegated to what was essentially a communications role subordinate to the ASH.
Over time, says Parascandola, officers became primarily responsible to the agencies by which they were employed, and were overseen by Corps leadership in largely an administrative capacity. There was small consolation in the fact that the ASH supervised the agencies that employed Corps officers, but even that changed in 1995, when another major reorganization shifted the oversight of those agencies to the Secretary of HHS.
As a result of these restructuring efforts, Corps officers now literally answered to two masters. Each officer had a boss at his or her day job, often a civilian government employee, whose chain of command led upward to a civilian HHS secretary. At the same time, the Surgeon General’s office oversaw their Corps-related duties and compliance with Corps requirements. The changes, Parascandola says, led to confusion within the agencies about whether the PHS as a division even existed anymore.
As the Corps’ command structure was weakened over the course of decades, so was its esprit de corps. Several Surgeons General tried to revitalize organizational morale within their limited scopes, but the internecine squabbles that resulted highlighted rifts among culturally and geographically disparate members of the Corps that had grown irredeemably deep.
Few issues highlight the challenges of uniting an organization under a diluted authority — and the internal culture clashes that chronically afflict the Corps — as starkly as the question of uniform wear. The Corps was founded as a uniformed service, but by the 1980s, with officers scattered across agencies and often surrounded by civilians, a growing number wore their uniforms rarely, if at all.
In 1982, when Surgeon General C. Everett Koop took office, uniform wear among officers was variable. When Koop declared he would require daily uniform wear in 1987, the backlash was fierce. In their coverage of the announcement, The Scientist magazine quoted an incensed virus researcher at the National Institutes of Health (NIH), who was dressed in jeans and sneakers: “I work with lab animals all day and they’re scared enough as it is.”

Surgeon General C. Everett Koop speaking at a news conference in 1986. When Koop declared he would require daily uniform wear a year later, the backlash was fierce.
Visual: Wally McNamee/Corbis via Getty Images
Eventually, Koop allowed agencies to set their own uniform requirements. When Scott Dowell joined the Corps as an Epidemic Intelligence Service (EIS) officer at the CDC in 1993, he wore the uniform per the agency standard, once a week. But in 2004, Surgeon General Richard Carmona, himself an Army veteran, changed the rules: officers were to wear uniforms whenever they were on duty. By the mid-2000s, officers were encouraged to deploy in uniform, says Dowell, who led the CDC’s division of Global Disease Detection and Emergency Response until 2012. “There was always this question about the funding of the Corps,” he said. But the response to be more visibly in uniform, Dowell said, was “a sort of gradual evolution.”
Some officers read uniform wear as a desperate performance aimed at placating those who feel the Corps does not deserve military status. “You wear the uniform that looks like a Navy officer, but you’re not Navy, you’re not in the military,” one officer told me, speaking anonymously out of concern for professional censure. “But then you get benefits like you’re in the military.” In some sense, the officer continued, people “try to be more military than military to justify the fact that they’re getting these benefits.”
But where some see desperation, others, especially those with a history of service in other uniformed organizations, see duty.
Michael Muni, an officer at the Health Resources and Services Administration who served as a police officer prior to joining the Corps, says his uniform is symbolic of the oath he took for his country. “This isn’t like an enlistment in the Army, where you sign a contract and you have to do so many years and you’re stuck wearing this uniform,” he says. “If somebody doesn’t want to wear this uniform, they don’t have to wear it.”
In other words, he means, they can leave.

Every decade or so, a government agency issues a report evaluating the Corps’ management practices. Often, irate legislators reduce or redirect the Corps’ funding in response; when they do, the Corps is incrementally weakened. The pattern started in 1962, with other reports published in 1971, 1982, and 1989. In 1996, the General Accounting Office issued a publication with the Damoclean title, “Federal Personnel: Issues on the Need for the Public Health Service’s Commissioned Corps.”
Ned Holland served as Assistant Secretary for Administration of HHS when a similarly critical report was finalized in 2010. He commissioned a financial supplement to the report, motivated largely by his hatred of bloat. “It’s non-partisan,” he said. “If you’re a conservative, you should want to save money because you want to save money. If you’re a liberal, you ought to want to save money so you can do more stuff.”
Before he worked for the federal government, Holland’s job was to trim the fat at Fortune 500 companies — “Get done the mission and save money doing it,” he said. After he was appointed at HHS, he asked the agency’s Office of Business Management and Transformation (OBMT) to evaluate the Commissioned Corps’ costs. The HHS report noted a decentralized organizational structure resulting in accountability gaps, detailing officer complaints about haphazard organizational communication and regressive information technology. Furthermore, the financial analysis concluded that considering differences in pay, retirement benefits, health care insurance coverage, and taxation, among other things, the Corps was costing the American taxpayer $217 million more annually than a civilian force would. The report recommended reorganizing Corps headquarters and consolidating resources, including multiple computerized personnel management systems.
Yes, many Corps officers do day jobs that a civilian could do, says James Currie, executive director of the Commissioned Officers Association of the U.S. Public Health Service, an advocacy and lobbying group for the organization. “But in addition to their day jobs, they keep what we call a ‘go bag’ next to the door so that when there’s a disaster, they go home and they pick up their stuff and they go to the airport with their orders in hand, and they fly to wherever they’re needed.”
The writers of the OBMT report had considered this. “The Corps is not the only asset within the Department to respond to emergency events,” it noted. In fact, civilians out-deployed Corps members to natural disasters between 2008 and 2010 by at least a factor of four. Many of those civilians were employees of other HHS agencies, but increasingly over the three-year period for which complete data is available, they were members of the clinically focused National Disaster Medical System (NDMS), a recently revitalized, rapidly deployable force of private-sector health care workers.
After accusations of mismanagement during Hurricane Katrina, the NDMS reorganized under HHS in the late-2000s and began increasing its deployments to public health emergencies. Compared with Corps officers and HHS civilians, NDMS employees accounted for at least 83 percent of the trips taken in response to the massive earthquake that shook Haiti in 2010. And, the OBMT report argued, they were faster to arrive and more clinically oriented than the Corps. As a deployment force, the report seemed to say, the Corps didn’t provide much bang for the buck. And if it wasn’t a deployment force, was it really worth keeping around?
Leadership at HHS appeared to take the report’s message to heart. In the budget request for fiscal year 2012, a line item to support team and readiness training for Corps officers decreased from $14.8 million to $7 million — and the following year, it was gone. And without money to pay for administrative salaries, staffing levels at headquarters fell. “We were supposed to have, for example, a major transition of our information technology components,” says Boris Lushniak, who served as Acting Surgeon General in 2013 and 2014. But “ultimately, it kind of fell to the wayside partially because we were not, you know, effectively funded.”

In testimony submitted to a Senate Committee on Appropriations in November of 2014, Currie wrote that the absence of funding to ensure proper training and equipment of Commissioned Corps officers flouted the law and negatively impacted teamwork: “PHS officers are fully engaged in day jobs which sharpen their clinical skills and make them eminently qualified in their specialty. What they do not have — because of a lack of training funds — is the benefit of training together as teams, getting to know each other, and working together in the field, as the military does regularly.” The $5 million that would be required annually to provide continued training for Corps officers was so small, he said, it would be “totally lost” in the HHS budget.
The OBMT report did not go unanswered: After its publication, the PHS Commissioned Officers Foundation for the Advancement of Public Health (PHSCOF), a nonprofit foundation that advocates for Corps interests and provides financial support for some of its programs, commissioned its own study. Published in 2013, it was a more qualitative and emotional analysis than the OBMT’s. “The effectiveness, efficiency, efficacy, and comprehensive value of the USPHS CC cannot be determined based on cost factors alone,” its first page declared in bold type. Even if the Corps were less cost-effective than its civilian equivalent, the report argued, it has advantages that justify its price tag.
The Corps does not pay for overtime, for example, which can add up: In 2017 alone, civilians deployed to hurricanes in Texas and the Caribbean earned as much as $120 million in overtime pay. Additionally, the Corps attracts more highly skilled professionals than civilian services. Corps nurses, for example, are required to have at least a bachelor’s degree in nursing, while only 50 percent of civil service nurses have bachelor’s degrees.
When he considers both the 2010 government report and the subsequent 2013 report commissioned by PHSCOF, Lushniak doesn’t really know which is more accurate, in part because he’s not sure anyone has the right data to make a fair comparison. But both reports identified something about the Corps that rang true: It is “so decentralized, so diluted as a uniformed service,” Lushniak said, “that people question it.”
In discussions about whether certain federal employees should be uniformed, there is an implicit understanding that the reward of wearing a uniform is military pay and benefits, and that the sacrifice is a degree of personal autonomy. Uniformed service members are expected to cede control over where and when they work — in other words, to live not where they want to live, but where they are told to live, and to deploy not when they feel like it, but when they are told to. Under this schema, the payoff for maintaining the Corps as a uniformed service should be a force geographically situated to meet the country’s most important day-to-day population health needs, and rapidly deployable in the event of more urgent public health demands.
President Trump’s “Reform Plan and Reorganization Recommendations” aims, among other things, to “transform the Commissioned Corps into a leaner and more efficient organization.”
Visual: The White House
It hasn’t worked out that way. When a person decides to join the Corps, Lushniak said, they must find a job before being commissioned into the Corps — “but you’re not going to get commissioned unless you find a job,” he said. And once in the Corps, officers change jobs and locations only when they elect to, rather than being assigned duty stations. Corps deployments, too, are similarly elective: Although the formal Corps position is that all officers are deployable, in practice, officers can simply decline to deploy for personal reasons.
The military does not have this problem; Armed forces deployments are less “can you” and more “you must.” That’s not necessarily because Corps officers are soft, said Lushniak, but because the armed forces have one chain of command, which is directly tied to who’s paying the bills. “No one else amongst the other six uniformed services — no one — has this number of issues resulting from a funding stream that is, one, very convoluted, and two, at times very precarious,” he said. Although the Department of Defense pays for everything for its service members out of money it is allocated in each year’s Congressional budget, Corps officers’ paychecks are scraped together from a bricolage of funding.
When the CDC hires a Corps officer, for example, it pays for that officer’s salary and relocation costs. Medical and retirement benefits are cobbled together from HHS funds administered by other divisions (though a new plan would see newly commissioned officers receive some retirement benefits from their employing agency itself) and administrative, logistical, and operational support costs are paid for by an overhead charge HHS levies on the agencies that employ them.
So many different sources pay for that officer, says Lushniak, that there’s enormous ambiguity about who their controlling authority is. “Unlike other uniformed services,” he says, “the big question is, who’s really your boss in the system?” That ambiguity means Corps leadership can’t get the right people into the right place at the right time, leading to criticism that the Corps is a non-effective responder, he says.
The Corps faces another obstacle when deploying clinical officers — nurses, doctors, psychologists, and others — on short notice to locations requiring direct patient care. As health care providers for underserved Americans, Corps clinicians are often “mission-critical,” meaning they are irreplaceable at the facilities where they perform their day jobs. In other words, those most capable of taking care of patients during a deployment are already needed to take care of patients back home.
Although Corps communications staff said all officers are deployable, a review of internal Corps data indicated that nearly 10 percent of all Corps personnel were classified as mission-critical in December 2016. It was unclear how many of these personnel had clinical day jobs. The latest HHS budget request indicates plans to address this issue with a Ready Reserve Corps of additional personnel.
The current voluntary nature of Corps deployability, however, along with the organization’s competing missions and its patchwork funding were thrown into sharp relief during the 2014 West African Ebola outbreak, when nearly 300 officers were mobilized to staff the Monrovia Medical Unit (MMU), a field hospital intended to serve health care workers in Liberia who may have been infected with Ebola. The goal of the mission was to remove barriers to doctors and nurses wanting to help, whether from Liberia or from abroad. By some accounts, Corps membership rose unequivocally to the occasion. “When they put out the word for volunteers to go to West Africa to deal with patients with Ebola — meaning that you were going to be exposed to this virus that had a very high lethality — I will say 5,000 Corps officers volunteered in the first week,” Currie, the Commissioned Officers Association leader, said. “They only needed 300. It totally overwhelmed the system.” Lushniak, the former acting surgeon general, asked: “Guess how many people we had to force to go to Liberia?” The answer? “Zero. Right?” he told me. “Every single officer there was a volunteer.”

Other recollections of the Liberia deployment, however, were less rosy. According to some people involved in the 2014 Ebola effort, a sufficient number of volunteers was, at least in the beginning, hard to come by, with many Corps members pushing back hard against deployment — and some initially refusing outright — citing the long stretches abroad and the possibility of quarantine on their return.
But the organization struggled to meet the personnel needs of the MMU for other reasons, too. Like many emergency-response clinical assignments, the MMU’s high level of care required staffing by doctors and nurses who were at the top of their games, with active, up-to-date clinical skills. But many of the officers with those skills were already mission-critical at their day jobs. The resulting “balancing act within some HHS agencies” was a challenge during the response, according to a 2016 report.
Additional delays resulted from a lack of funds to train the officers, all of whom needed specialized training in “donning and doffing” — getting into and out of the suits that would protect them from becoming infected. The Corps didn’t have the resources to send officers to the three-day preparatory course offered by the CDC in Anniston, Alabama. For weeks, it was unclear if and how any of the hundreds of officers would be trained, a senior CDC official familiar with the events told me. (The official spoke on the condition of anonymity out of concern for repercussions against colleagues.) Eventually, funds from the CDC and HHS paid for the Corps officers’ training.
Although discussions about deploying Corps officers to staff the MMU began in August or September of 2014, the unit did not open until November of that year. The delays likely significantly reduced the impact of the 25-bed unit, which opened after the epidemic peaked: In total, over the six months it was open, the facility provided care for 42 patients — less than 15 percent of the nearly 300 Liberian health care workers believed to be infected through March 2015.
The MMU “would be the thing that contributed the least to the outbreak control,” said a CDC official with knowledge of the outbreak response, who spoke on the condition of anonymity out of concern for professional repercussions. Nine hundred other Corps officers were deployed for non-clinical outbreak response work in Sierra Leone, Guinea, and Liberia, as well as to U.S. airports to staff quarantine stations; the MMU’s impact on the outbreak “was minimal compared to the thousands and thousands of hours that CDC Commissioned Corps officers spent in those three countries doing contact tracing and infection control and all those other outbreak investigations,” said the official.
The CDC is, after all, the federal agency responsible for epidemic investigation and control. “If the Corps made any impact on the Ebola outbreak,” the official said, “it was through that and not through the MMU.”
Not all of the impact of a disaster response can be measured by the trajectory of an epidemic: The Corps was the only U.S. government entity providing direct patient care during the Ebola outbreak in West Africa — part of “a critical example of American leadership,” as President Obama remarked in September 2015 on presenting a Presidential Unit Citation to Corps officers. Furthermore, according to former HHS and PHS officials, ensuring a high level of medical care would be available if health care workers themselves became infected likely elicited help from other governments and increased chances the U.S. would be on the front lines of future outbreaks of international consequence.
Since 2006, Corps leadership has been making changes to improve the organization’s deployability, among them the implementation of rapid deployment forces teams, each consisting of 150 officers and able to deploy within 12 hours of notification. Each is on call one of every five months, although, said Lushniak, “at the end of the day, the sense was that, well, this is still considered somewhat an optional agreement.”
Perhaps because of its “can you” approach, the Corps attracts a certain set of people who like the structure and benefits of the armed forces, but also like stability. An officer who transferred to the Corps after several years in the Army — he calls himself an “unofficial recruiter” for the Corps of people looking to leave the Department of Defense — said Corps officers’ personal autonomy is a big selling point for military personnel.
Want more Undark? Subscribe to our weekly newsletter!
Speaking anonymously out of concern for professional reprimand, officers with prior armed forces experience said some differences between the organizations are less appealing. The Corps used fax machines to collect personnel data until late 2016, and the transition to their replacement systems did not go smoothly; some officers have been denied candidacy for promotion and threatened with involuntary separation because documents they had uploaded were lost due to software glitches. In early 2018, an administrative oversight resulted in abrupt and well-publicized temporary pay cuts for thousands of officers.
Corps promotion benchmarks include something called “officership,” broadly translating to extracurricular activities promoting Corps visibility and weighted at 15 percent of a promotion package. One officer described a colleague’s “major brownie points” for singing in the Corps’ choir.
“Army would laugh if I ever tried to have that count,” he told me. Another officer observed: “In the military, doing your job was your service to the Army. But in the Corps, it seems more and more that’s not really the case.”
Even in the face of the Corps’ unwieldiness, there is a contingent that insists that without it, portions of the American public health infrastructure would suffer.
Among them is Mary Smith, who led the Indian Health Service (IHS) from March 2016 into 2017. The agency has for decades had difficulty recruiting clinical staff to work in its facilities, many of which are on tribal lands in remote areas with limited housing and transportation options. As a consequence, facilities are chronically understaffed; nationally, said Smith, the IHS averages a 20 percent vacancy rate among its medical staff positions.
Nearly 2,000 of IHS’ 15,000 employees are Corps officers, many of whom are drawn to the agency by the opportunity it offers to care for underserved populations while receiving military benefits and above-average pay. Being able to offer Corps pay and benefits as part of hiring packages “was a distinct advantage because that allowed possibly being able to fill a position that otherwise might not be filled,” said Smith. She fears even more posts would be left vacant if the agency lost the incentives the Corps provides. “IHS has severe hiring challenges,” said Smith. If the Corps’ numbers were radically reduced, “those challenges would just become exacerbated,” she said.

More of the Corps’ workforce is employed at IHS than at any other federal agency. In second place is the Food and Drug Administration, and in third is the CDC, which as of July 2018 employed more than 900 Corps officers at posts both U.S.-based and international. The CDC’s mandate arguably aligns more closely with the Corps’ than does any other agency’s: both have the same broad public health mission, and the CDC is one of the few agencies that routinely deploys people to public health emergencies. Like IHS, the CDC relies on the Corps to attract and retain high-caliber public health experts and “has been an attractive place to go — in part because of the Commissioned Corps and the salary and other benefits,” said Scott Dowell.
“It wouldn’t take much to compromise that,” he added.
One of the biggest agency-side advantages to employing Corps officers, regardless of which agency is the employer, is that officers are “on duty 24/7” — not just for the Corps, but for their agency. That translates to long overtime hours without additional compensation, which is particularly cost-effective for the CDC during outbreak scenarios. “I think the military structure and the Commissioned Corps’ rules enabled CDC Commissioned Corps’ officers to do what they do best, which is to be highly trained, adequately compensated people who can deploy any time to crisis situations,” he said, and employing Corps officers at CDC builds deployment and preparedness into the organization’s culture.
With a diminished Corps, Dowell fears the CDC would not be able to recruit the expertise it currently does, nor respond to either domestic or global health emergencies with its current speed and expertise. “I think that’s the biggest threat to national security, is that the result of this kind of thing will be that the quality of CDC’s first-line outbreak responders will be diminished slightly and therefore, they will no longer be on the front lines of responses,” he said.
Various government reports published over the last half century suggest the Corps’ work can be done for less money by employing civilians to do the work officers do. But dollar amounts don’t measure quality, argue proponents of preserving the Corps: If you try to hire people to do the Corps’ work while paying them civil service pay and benefits, you simply won’t get the same people.
Before the Trump administration’s OMB proposed reducing the size of the Corps, it first proposed eliminating the Corps entirely. Corps officer and cardiologist Brian Lewis, who chairs a committee representing Corps physicians, explained to his membership why that didn’t happen in a January 2019 newsletter: Current U.S. Surgeon General Dr. Jerome Adams “advocated for OMB to allow the Corps to survive. His efforts avoided the Corps’ demise,” he wrote.

In response to Adams’ advocacy, OMB instead recommended widespread cuts to the Corps through changes including personnel reductions, creation of a Ready Reserve Corps, and reassigning of costs. The proposal, made as part of a 128-page public document proposing government-wide cuts last June, was followed by a small deluge of internal directives from the office of the ASH, each causing a fresh wave of panic among Corps membership. The changes causing the greatest concern are those that seem engineered to push out clinically-trained officers working desk jobs, often by tying a large portion of their salaries to a newly added clinical work requirement.
One of the most controversial new policies will require these officers — like, for example, the hundreds of physicians who work at the CDC — to perform a minimum of 80 hours of patient care annually to receive their current salaries, though the Surgeon General can waive this requirement in certain cases. For officers who haven’t worked at the bedside for years, re-entering the world of clinical practice is enormously challenging — and some may opt to leave the Corps rather than try.
That may be the point, said John Parascandola, the former PHS historian, who is concerned about the Corps being “nickeled and dimed to death.” Eventually, Parascandola said, the incremental drainage of funds and personnel as a result of small policy changes will weaken the Corps to the point critics can say “‘Well, what are they doing? You know, they’re not getting their job done.’” The fewer resources there are for the Corps to accomplish its mission, the easier it will be to argue its work can be done by someone else.
But what is that mission, after all? Corps officers themselves seem unsure: In a November survey, Corps physicians said an uncertain mission and identity was the most urgent challenge facing the Public Health Service.
The Department of Health and Human Services has noted that the Corps is undergoing a far-reaching reevaluation of its structure, strengths, and costs. However, few specifics have been released to the public and by some accounts, information shared within the Corps also remains limited. In a December 2018 newsletter to members, John McElligott, the deputy executive director of the Commissioned Officers Association of the U.S. Public Health Service, expressed frustration with the silence of HHS leadership: “This information should really be coming from HHS,” he wrote, “but, from what we can tell, the Department is not sharing much about the future direction of its uniformed service.”
In a January, 2019 newsletter, Lewis suggested that there was “light in the darkness.” Included in the ongoing evaluation, he noted, was “[a] rethinking of the Corps mission based on what we already do well, much of which is asked of us by the Nation.”
No one really knows what the Corps could accomplish if it were given a military-style chain of command and a military-grade budget to match its military model. The organization currently compensates its officers like they’re in the military; what if it recruited and deployed them that way?
Lushniak imagines a service where, as in the other uniformed services, newly commissioned officers go where they’re needed — and where they’re told. If new Corps officers were assigned to, say, Sitka, Alaska for their first two years, he said, “is that going to work to our benefit or detriment? I don’t know.”
Ned Holland, formerly of HHS, is less ambivalent. “The central purpose of the military is different than the central purpose of the Department of Health Human Services,” he said, “and there are reasons to adopt and utilize the cultural methodologies of the military. The question is whether those apply to the people who provide public health support.”
If you ignore for a moment the uniquely American link between military service and the guarantee of good health insurance, affordable education, and a retirement plan, expecting a military model to add value to a public health force just doesn’t make sense, Holland told me. Emergency response is in the DNA of public health culture; people in public health run toward emergencies the way soldiers run into opposing fire, regardless of whether they’re uniformed or not. The CDC, Doctors Without Borders, and countless volunteer organizations have not needed military structure to respond selflessly, efficiently, effectively, and frequently to emergencies.
More Corps members serve the Indian Health Service than any other agency, and defenders say that Native American public health infrastructure would suffer if the Corps were disbanded. Above, Dr. Ty Reidhead, Director of the Indian Health Service Phoenix Area.
Visual: U.S. Department of Health and Human Services
Clinicians driven by a sense of justice likewise run to where the gaps in health care are widest, some Corps observers have said, and they don’t need a military structure to incentivize or enable them to serve the underserved. What they do need is enough money to take as good care of themselves and their families as they do their communities. “The Commissioned Corps’ people are skilled, able, and dedicated, but I think the Corps concept is an anachronism,” says Holland. “And you can get their skill, ability, and dedication without uniforms and without the attendant additional expense.”
Ian Norton, who leads the development of emergency medical teams at the World Health Organization, remembers being at an international meeting when a CDC representative said something like, “We believe in separating clinical and public health emergency response teams.”
Norton thought it was a “rich-country statement.” Representatives from Nigeria, Sierra Leone, and the Solomon Islands expressed the room’s consensus: Separating emergency medical teams along clinical and non-clinical lines is ludicrous.
Although emergencies do require people to provide direct patient care, they also require people to find and quantify health needs; conduct surveillance for diseases that accompany infrastructure disruptions and crowding; manage and report data that’s collected; and identify and contain outbreaks of infectious disease. These are vital epidemiological tasks, but they are not clinical duties. And a response team is only as good as “what wraps them in bubble wrap,” says Norton, referring to the operations and logistics personnel who determine how fast the team arrives, who feeds and waters them, and where they get the tools they need to make the team work.
Speed and training matter, too. A team’s door-to-disaster time can make a big impact on the number of lives it saves. Military teams or teams that partner with military units for transport usually arrive earlier and can respond more effectively. It is standard for teams to train together before deployment in order to minimize glitches when the stakes are high.
Most other countries rely on multiple organizations to accomplish what the Public Health Service tries to do as one, and on a shoestring. Few people would disagree that it’s important to have a public health infrastructure in place to care for patients in parts of the U.S. where it’s difficult to live, to respond quickly to emergencies and natural disasters, and to do the day-to-day work of preserving and protecting the public’s health. But should all of these responsibilities be assigned to a single organization? And does the uniform and its attendant structures facilitate or impede the fulfillment of those responsibilities?

At least one country has seen remotely stationed public health workers as the solution — rather than the problem — in emergency response. After the 2010 earthquake in Haiti, the first people Norton’s team approached when recruiting for the Australian Medical Assistance Team (AusMAT) were those with experience working in the Aboriginal community. “I feel those who work day-to-day in less privileged circumstances do better,” he said. Deployments are usually short, just a few weeks, and voluntary. When the responder deploys, the same national authority that deployed them pays their employer enough to hire a temporary worker to backfill their spot.
The system works; deployment is now used as an incentive to draw providers to remote, rural posts, and is not seen a drag on the country’s national health system. The parallels are clear: By adding a centralized chain of command and funds, Australia turned an understaffed, remote health care system and a need for nimble disaster response into one of the world’s leading emergency medical teams. Could the Corps innovate like this one day? Maybe — but it has bigger concerns right now, Lushniak suggested. “We’re going through yet another phase, which is the OMB and the current administration’s want and need to once again look at this model and say, ‘Something’s wrong with this model,’” he told me. The response of the current administration, he says, is to decrease the size of the Corps.
But decreasing its size isn’t the answer, or even the issue. “It’s, I think, a more simple question,” Lushniak said. “Do you want this model or not?”
Adam Lofton has a ready answer to that question. When he was deployed to Puerto Rico in 2017 to stand up medical shelters for people with chronic health conditions following Hurricane Maria, his team identified a coliseum ideal for housing the shelter except for its lack of running water. After finding the facility’s pump station, Lofton and other Corps engineers met with local officials to get downed power lines and vegetation cleared from the road — the trees were so brown and bare, it looked like southern Texas, he said. From there, they were able to work with the U.S. Army Corps of Engineers to turn the pump back on.
Not long after hearing the loud hum of the water rump roaring to life, Lofton, now back at the coliseum, began hearing the voices of local residents talking in Spanish. It took him a while to understand what they were saying, but when he did, the hair on his arms and the back of his neck stood up. “We’ve got water,” they were saying. Fixing the pump station had restored water not only to the coliseum, but also to 25,000 homes in the region.
This year will be Lofton’s 15th in the Corps, and he knows political support for the organization ebbs and flows. But in his view, what the Corps does makes it too critical to the country to just be eliminated on a whim. So he doesn’t worry about it.
“I’m just excited to be a part of it,” he said, “and have faith that because it is needed, it’ll always be there in some way or another.”
Keren Landman is a practicing physician and writer who covers topics in medicine and public health. Her work has appeared in Vice, STAT, and the Atlantic, among other publications.
Comments are automatically closed one year after article publication. Archived comments are below.
So…..where the hell is the USPHS Commissioned Corps during this crisis? The entire organization should be mobilized and all clinical personnel deployed…but are they. NO!
I am a previous active-duty USPHS Officer (senior officer), with eight years of active-duty service in the regular Air Force biomedical service corps. My time in the USPHS was divided in the Federal Bureau of Prisons (prison hospital) for five years and the Rockville/D.C. headquarters for the remainder.
I eye-witnessed countless cringe-worthy instances that provided grand opportunity for pause. Promotions to Admiral (0-7/0-8 rank) of political friends of whomever was in the WH or a chamber of Congress…some who were long-term USPHS Corps officers, others were literally civilians the day before pinning on one or two stars…the only officer with three stars is the Surgeon General, who is traditionally a civilian the day before, and the only officer with four stars is the Assistant Secretary for Health who is ALWAYS a civilian the day before. How cringe-worthy is that? We would promote some officers to 0-6 (full Colonel rank) at 8-10 years of service…cringe away, that happened on the regular.
The PHS Commissioned Corps has no resources, money, equipment or supplies, no vehicles…cars, trucks, planes, helicopters, boats, or ships (historically, we’ve had all of those), no bases (not even a donated closed base), no warehouses, no training funds, no hospitals (historically, we’ve had hospitals, quarantine stations, and immigration ports like Ellis Island)…we literally have nothing.
As a former PHS Officer I can tell you first hand that the USPHS Commissioned Corps needs a severe restructuring. There isn’t enough space here for me to really expand on my observations, but suffice to say the USPHS CC needs an overhaul.
A large percentage of PHS officers are sitting in office jobs that could very easily be held by civilians. Jobs like FDA, and CMS compliance inspectors.
Also, the officers in the Washington/Rockville area and CDC made damn sure they stack the deck to ensure their promotability. Seriously, how can a commissioned officer (podiatrist) join the organization as an O3 and be promoted all the way to O6 and never been assigned to a clinical position let alone anywhere outside of the Rockville area? There are many officers similar to this. The USPHS is also extremely top heavy.
The USPHS needs to be removed from DHHS and absorbed into the medical command structure of one of the military branches and subject to the UCMJ.
How do I get copy of my USPHS discharge papers
I really don’t see the need for this organization. They get same benefits as our armed forces and do not have to deploy or do anything combat related. I think the government transition this organization into the Navy National Gaurd or Reserves. This organization is a slap in the face to our armed forces. If you want to wear the uniform join the military. Fema and the National Guard handles the majority of this stuff anyway and they can deploy to fulfill military duties
I am a current PHS Officer, proudly serving a critical role in my agency and leading a deployment team. My fellow Officers and I have responded to mass shootings, hurricanes, floods, tornadoes, disease outbreaks and many other disasters, working around the clock to meet the mission and serve vulnerable populations. The main problem is not the Officers, but the agencies and supervisors within the agencies, which can deny an Officer the opportunity to deploy because of short staffing, or just because it is inconvenient. For the PHS to be most effective, there needs to be restructuring which allows Officers real deployment “orders” that can’t be vetoed by a first or second-line supervisor, just as Reservists in military branches are allowed to deploy in the event of an emergency. In our agencies, we regularly take on additional duties and do so with pride. Those who feel we are not an effective use of taxpayer dollars likely haven’t served as a PHS Officer or had a bad experience (it can happen with a poor supervisor). Personally, I wouldn’t trade my role for any other public or private sector job. We promote, protect and defend the health and safety of the nation with integrity each and every day.
PHS needs to be restructured and actually do what they say they’re going to do (i.e. help out where healthcare is needed), or it needs to be done away with. Plain and simple. The Corps is inefficient and many of its functions are carried out by more competent entities like NDMS. It currently does not merit military benefits given that none of the officers are sent where they are actually needed. They get to apply to jobs like civil servants and ask their supervisors to deploy for a measly two weeks. Many other civil servants deploy for longer periods. It’s time to restructure or trim the fat!
All of our institutions are under attack and have been for decades. The health industry views any agency like this as a direct threat. We are seeing epidemics of diabetes, drug addictions, and suicides, yet there has been no public health response. In fact we have seen an industry response of monetizing every aspect of this. Like every other beneficial government program, they have been deliberately decapitated, under funded and have had any authority undermined.
The great majority of Americans believe, that the government is tracking their every move, and that public health issues would be identified. Instead the only tracking done anymore is to improve industry profits. These industries had to undermine our public health institutions, after all it has been profitable. The PHS would have recommended years ago, a Universal Health Plan, to protect all Americans. Instead we got the badly undermined and eviscerated ACA.
We are all being Gas Lighted by the industries, that are profiting from our bad health. They undermined any government agency that could have challenged them, while the media runs a false narrative about government over reach. The very government institutions that were supposed to protect us were either undermined or taken over by the industries. This country used to have laws about health marketing, because sick people are vulnerable to false claims. Now this marketing has been weaponized, with many media outlets depending on the very profitable health industry for advertising revenue. The very day our congress met to discuss prescription drug pricing, the industry ran adverting to attack the questioning.
We are seeing the result of corrupt unregulated capitalism, years of regulatory capture, industry insiders at federal agencies, and corrupt lobbying practices. At the same time the media runs a counter narrative to protect these industries on every level. They bellow the words “Big Government” while the government agencies that were supposed to protect us, have less staff than 30 years ago. With the current administration the fix is in, as industry insiders take over every agency, with an agenda of destroy or profit.
The Anti Vaxx Movement, should have been a wake up call. They spread that nonsense because it was profitable. The FTC have been eviscerated, and is unable to recognize the deceptive health marketing. The laws were in place for a reason. We have been relatively lucky that we have not had a real serious outbreak, Measles was serious enough. There is a clear failure in our health industry, leading millions of people to alternatives. Since there is no scientific based public health agency, there has been no tracking of the adverse events and negative outcomes. Time after time we find out that the agencies not only failed, but took industry money to exploit us all. As our population grows, it is even more imperative to have a functioning public health service.
I was in DHHS after serving (with outstanding references) in both Senate and House. At first I was elated because Surgeon General Bennett assembled a small group of experts charged with reforming the department. But he resigned within the year, and he group scattered. I stayed on, only to see one agency created after another, fully staffed, but not funded to actually do anything – for example, the agency for health manpower. Finally I landed a PASA assignment with State Dept., and for the next ten years I created health systems in countries abroad – for example, Korea and Thialand – and rose to the highest nonsupervisory rank. Then it ended, and I was shuttled back under newly appointed SG C. Everett Koop. He, his Deputy Faye Abdellah and PHS employees were not only absolute clods, they engaged in illegal, destructive and hurtful activities with abandon. PHS doctors held positions that could be filled by civil servants making $10,000 less. The lied extensively and profusely, some of them boasting about methods of firing civil servants and setting the up for that purpose. And they accomplished no work worth performing. I quit in 1987 to accept a Fulbright professorship in Papua New Guinea, badly scarred but happy to be free. I regret ever having thought that PHS or DHHS were able capable of being of benefit to patients in the US or abroad, and I see no reason for their continued existence.
I served honorably in the US Army and the Commissioned Corps I complained about triaging diagnosing and prescribing medication to patients and within twelve weeks I was kicked out of the Commissioned Corps. “There can be no appeal and no review of this decision”.
I appealed to the USPHS Board for Corrections and received seven spent 9mm bullet casings in a USPHS envelope.
The USPHS Board voted, twice, unanimously in my favor. USPHS ‘non-concured’.
I appealed. An Assistant Director of HHS, Mike Blank, said NO
The Army called me back up for Operation Iraqi Freedom.
I was not able to discover how I was called back to the Army if I was a kicked out Commissioned Corps officer. I went to two Federal courts and the Supreme Court (16-8208). Case not accepted.
I still wonder how the USPHS can hand out Commissions on behalf of the government without explaining what happens to a Commission at termination of Service.
Why was I kicked out? “You do not have the necessary discipline and dedication to duty to be a Commissioned Officer for the United States of America”.
I served my country with honor and distinction in peace and war, and THIS is how I was treated! I want that stigma the USPHS attached to my name erased, but how? To me the honor of my name is worth any wait and work, but how to fight the USPHS?
Regarding firing: (my stories are all from the Indian Health Service). A nurse was one week away from completing whatever time it is that Civil Service personnel have to do to get a permanent job. She was well liked, had good evaluations, and loved her simple life on that Reservation. Her bosses boss said to fire her the day before she would complete that time period. The direct boss refused, so the other one brought her the papers. Naturally she was devastated. It was really cruel.
Also at that Service Unit we had a young female Vietnamese-American Resident from UCLA doing a rotation. She was smart, lively, sporty with a great sense of humor and the Tribal members liked her a lot (especially the EMT’s-I did several ambulance runs with her and I saw their interactions first hand). A couple of months after she went back to finish at UCLA she called me in tears. She told me that the doctors at that Service Unit (Corps officers) had given her an evaluation that landed her in hot water with her professors. All of us nurses had enjoyed working with her, and thought she was one of the best that ever rotated through there. I simply don’t understand it. I hope she is a rich respected, beloved physician wherever she is now!